Anda mungkin juga menyukai
- Tips On Reducing Laboratory Plastic WasteDokumen13 halamanTips On Reducing Laboratory Plastic Wastekate2494Belum ada peringkat
- Sarstedt Environmental PolicyDokumen2 halamanSarstedt Environmental Policykate2494Belum ada peringkat
- The Social and Environmental Impact of Engineering SolutionsDokumen14 halamanThe Social and Environmental Impact of Engineering Solutionskate2494Belum ada peringkat
- Villa Nova-2016 Green Lab ProgramDokumen16 halamanVilla Nova-2016 Green Lab Programkate2494Belum ada peringkat
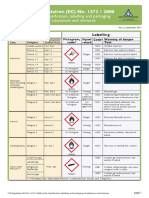
- SDS Hazchem Info SheetDokumen4 halamanSDS Hazchem Info SheetMartha FriaBelum ada peringkat
- Fumecupboard Sticker PDFDokumen1 halamanFumecupboard Sticker PDFkate2494Belum ada peringkat
- Laboratory Safety SymbolsDokumen5 halamanLaboratory Safety Symbolskate2494100% (1)
- GreenSeal ProductsDokumen23 halamanGreenSeal Productskate2494Belum ada peringkat
- Sash Stickers GreenLabsDokumen4 halamanSash Stickers GreenLabskate2494Belum ada peringkat
- Sigma SaponinDokumen3 halamanSigma Saponinkate2494Belum ada peringkat
- Claps 2017 Adding Metyrapone To Chemotherapy Plus Mitotane For Cushing's Syndrome Due To Advanced Adrenocortical CarcinomaDokumen4 halamanClaps 2017 Adding Metyrapone To Chemotherapy Plus Mitotane For Cushing's Syndrome Due To Advanced Adrenocortical Carcinomakate2494Belum ada peringkat
- Multicolor Flow Staining ProtocolDokumen3 halamanMulticolor Flow Staining Protocolkate2494Belum ada peringkat
- Sigma TO-901317Dokumen1 halamanSigma TO-901317kate2494Belum ada peringkat
- ShRNA ProtocolDokumen1 halamanShRNA Protocolkate2494Belum ada peringkat
- You Are Mine PDFDokumen2 halamanYou Are Mine PDFkate2494Belum ada peringkat
- UKCAT OfficialGuide 2015Dokumen84 halamanUKCAT OfficialGuide 2015kate2494Belum ada peringkat
- UN3373 Biological Substance, Category B Packed in Dry Ice by Air Authority LetterDokumen1 halamanUN3373 Biological Substance, Category B Packed in Dry Ice by Air Authority Letterkate2494Belum ada peringkat
- Sigma TO-901317Dokumen1 halamanSigma TO-901317kate2494Belum ada peringkat
- Sigma Aldrich ForskolinDokumen2 halamanSigma Aldrich Forskolinkate2494Belum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Vector-Borne Disease Management ProgrammesDokumen44 halamanVector-Borne Disease Management ProgrammesInternational Association of Oil and Gas Producers100% (1)
- The Kidney and Heart in CM - Part 2Dokumen7 halamanThe Kidney and Heart in CM - Part 2davidg2012Belum ada peringkat
- Physical Assessment DaraDokumen3 halamanPhysical Assessment DaraMichael Bon MargajaBelum ada peringkat
- Icd 10 - Penyakit Gigi Dan Mulut BpjsDokumen2 halamanIcd 10 - Penyakit Gigi Dan Mulut BpjsAdicakra Sutan0% (1)
- Rodent OncologyDokumen24 halamanRodent Oncology黃皓Belum ada peringkat
- Lower Motor Neuron LesionsDokumen29 halamanLower Motor Neuron LesionsLoshi ChandrasekarBelum ada peringkat
- Neurobiology of Post Traumatic Stress Disorder - Newport & NemeroffDokumen9 halamanNeurobiology of Post Traumatic Stress Disorder - Newport & NemeroffunonguyBelum ada peringkat
- Asphyxia by SuffocationDokumen15 halamanAsphyxia by SuffocationBryan Christopher Co Lao100% (1)
- 2002 178 181 Greguric Vucevac History EradicationDokumen11 halaman2002 178 181 Greguric Vucevac History EradicationDalen OdobašićBelum ada peringkat
- LeptospirosisDokumen40 halamanLeptospirosistummalapalli venkateswara rao86% (7)
- Development of VeinsDokumen37 halamanDevelopment of Veinsokolodivine334Belum ada peringkat
- Benign Ovarian ConditionsDokumen31 halamanBenign Ovarian ConditionsNur Hanani KhanBelum ada peringkat
- Discrepancy Index Worksheet For Print PDFDokumen1 halamanDiscrepancy Index Worksheet For Print PDFTatiBelum ada peringkat
- Biology Today and Tomorrow With Physiology 5th Edition Starr Test BankDokumen24 halamanBiology Today and Tomorrow With Physiology 5th Edition Starr Test Bankdariusadele6ncs100% (33)
- Alteration in Endocrine SystemDokumen215 halamanAlteration in Endocrine Systemyen1988100% (1)
- Fluid and Acid-Base Balance Soca Devina CiayadiDokumen65 halamanFluid and Acid-Base Balance Soca Devina CiayadiDevina CiayadiBelum ada peringkat
- Bio Immune Gas Exchange MarkschemeDokumen4 halamanBio Immune Gas Exchange Markschemeyt kBelum ada peringkat
- 22Dokumen88 halaman22Resvian RemboyBelum ada peringkat
- Aciar113 PDFDokumen272 halamanAciar113 PDFfelinsiamelvanBelum ada peringkat
- Ch.8 - Axial & Appendicular SkeletonDokumen72 halamanCh.8 - Axial & Appendicular SkeletonMeganBelum ada peringkat
- Title: Healing Paws and Feathers: A Comprehensive Exploration of A Career in Veterinary MedicineDokumen3 halamanTitle: Healing Paws and Feathers: A Comprehensive Exploration of A Career in Veterinary MedicineDelia Maria VisanBelum ada peringkat
- Delta Green - Autopsy of A Sand DwellerDokumen2 halamanDelta Green - Autopsy of A Sand DwellerLuca LiperiBelum ada peringkat
- Si 68-71 Tatlife Layout 1Dokumen2 halamanSi 68-71 Tatlife Layout 1api-292331390Belum ada peringkat
- Livestock Superviser Job Description JB SDDokumen2 halamanLivestock Superviser Job Description JB SDSkyBelum ada peringkat
- Full Download Test Bank For Comprehensive Radiographic Pathology 6th Edition by Eisenberg PDF Full ChapterDokumen36 halamanFull Download Test Bank For Comprehensive Radiographic Pathology 6th Edition by Eisenberg PDF Full Chapterdiesnongolgothatsczx100% (13)
- Class 9 Economics Project On ToothpasteDokumen12 halamanClass 9 Economics Project On ToothpastePankajkumar GuptaBelum ada peringkat
- Science Workbook 1 Answers PDFDokumen26 halamanScience Workbook 1 Answers PDFทิตยา จิรกาวสานBelum ada peringkat
- NCERT Class 11 Biology Book ChangesDokumen8 halamanNCERT Class 11 Biology Book ChangesmurukesanBelum ada peringkat
- Manuscript Provisional PDF: An Unusual Cause of HypertensionDokumen3 halamanManuscript Provisional PDF: An Unusual Cause of HypertensionjoelrequenaBelum ada peringkat
- Debelica2009 AtlasKeyHairTerrestTexasMammalsDokumen108 halamanDebelica2009 AtlasKeyHairTerrestTexasMammalsJorge Manuel Cardenas CallirgosBelum ada peringkat