Anda mungkin juga menyukai
- PTW RenyDokumen8 halamanPTW RenyDarwin OlivaBelum ada peringkat
- Safety Handbook 2004Dokumen72 halamanSafety Handbook 2004ramibadranBelum ada peringkat
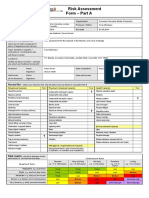
- Risk AssessmentDokumen2 halamanRisk AssessmentFaraiMbudaya0% (1)
- Centre WISP OSHA FinesDokumen14 halamanCentre WISP OSHA FinesRyan GraffiusBelum ada peringkat
- 20 Rules of Closing A Deal PDFDokumen21 halaman20 Rules of Closing A Deal PDFbioarquitectura100% (9)
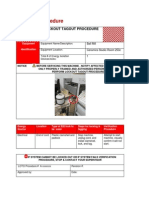
- Loto Standard Operating Procedure Sop - Loto - : Lockout PointsDokumen2 halamanLoto Standard Operating Procedure Sop - Loto - : Lockout PointsK3L ULP Tanjung RedebBelum ada peringkat
- Risk assessment for hanging doorsDokumen11 halamanRisk assessment for hanging doorsMitchRappBelum ada peringkat
- Lecture 3 - Process SafetyDokumen79 halamanLecture 3 - Process SafetyDivyashini MohanBelum ada peringkat
- Task Risk Assessment FormDokumen8 halamanTask Risk Assessment FormNurpadmi KusbiantoroBelum ada peringkat
- Activity 3.2.1 Training Needs Analysis (Dokumen1 halamanActivity 3.2.1 Training Needs Analysis (Mahnoor MasroorBelum ada peringkat
- OHS 5.3.1aPreventiveandCorrectiveActionFormDokumen1 halamanOHS 5.3.1aPreventiveandCorrectiveActionFormfcleong69Belum ada peringkat
- 21WN3K - 21WN9KDokumen2 halaman21WN3K - 21WN9KbioarquitecturaBelum ada peringkat
- Contractor Ehs Risk Assessment For NDT TestingDokumen6 halamanContractor Ehs Risk Assessment For NDT TestingBernard PenuliarBelum ada peringkat
- Form Pengeluaran Apd (Ppe Issued Form) : Pt. Hana Nuansa PratamaDokumen1 halamanForm Pengeluaran Apd (Ppe Issued Form) : Pt. Hana Nuansa PratamaAndi Rogers Sitepu100% (1)
- Cutting and welding safetyDokumen2 halamanCutting and welding safetyZaki ChaabnaBelum ada peringkat
- OHS&W Plant Specific Hazard IdentificationDokumen3 halamanOHS&W Plant Specific Hazard IdentificationJulio Best SetiyawanBelum ada peringkat
- Ge 9900Dokumen16 halamanGe 9900cernyjanek0% (2)
- Behavior Based SafetyDokumen14 halamanBehavior Based SafetyJody100% (3)
- Steel Structure WorkDokumen9 halamanSteel Structure Workmohd firdaus100% (1)
- 4.5.3!01!06 First Aid Property Environmental ReportDokumen4 halaman4.5.3!01!06 First Aid Property Environmental Reportloveson709Belum ada peringkat
- PPE Training ENGDokumen26 halamanPPE Training ENGfaik395Belum ada peringkat
- RA Excavation For Trial TrenchDokumen9 halamanRA Excavation For Trial TrenchSasi KumarBelum ada peringkat
- OSHA Sustainability PaperDokumen39 halamanOSHA Sustainability PaperbarhoumsrasraBelum ada peringkat
- Planned Job Observation Plan (Schedule) : Project Name: 380Kv DC Ohtl in Qiddiya Area ELEMENT 5.20.1Dokumen4 halamanPlanned Job Observation Plan (Schedule) : Project Name: 380Kv DC Ohtl in Qiddiya Area ELEMENT 5.20.1Shafie Zubier100% (1)
- HSE Campiagn - Safety Talk-01Dokumen2 halamanHSE Campiagn - Safety Talk-01NeeleshSoganiBelum ada peringkat
- 10 Tips Refrigerant PipingDokumen3 halaman10 Tips Refrigerant PipingAndres CarrascoBelum ada peringkat
- NR 18 - Aerial Lifts For ConstructionDokumen44 halamanNR 18 - Aerial Lifts For ConstructionCPSSTBelum ada peringkat
- Fire Protection Design Manual: Department of Veterans AffairsDokumen71 halamanFire Protection Design Manual: Department of Veterans AffairsmitasyahuBelum ada peringkat
- Safety and Health Committee OSHA 1994. Safety and Health Officer SHO Malaysia. Mesyuarat Jawatankuasa Keselamatan Dan Kesihatan Pekerjaan. JKKP 1996Dokumen25 halamanSafety and Health Committee OSHA 1994. Safety and Health Officer SHO Malaysia. Mesyuarat Jawatankuasa Keselamatan Dan Kesihatan Pekerjaan. JKKP 1996Zainorin Ali100% (8)
- IntelliROL IOM 90480001 r06092015Dokumen126 halamanIntelliROL IOM 90480001 r06092015Dropet Victor100% (1)
- Ladder SafetyDokumen2 halamanLadder Safetyavinash_mokashi7073Belum ada peringkat
- All FormsDokumen18 halamanAll FormsSuhendraBelum ada peringkat
- OSHA Safety and Health Program GuidelinesDokumen44 halamanOSHA Safety and Health Program GuidelinesNavindranPalasendaramBelum ada peringkat
- Ohs-Pr-09-03-F10 (A) Planned Job Observation ReportDokumen1 halamanOhs-Pr-09-03-F10 (A) Planned Job Observation ReportShafie ZubierBelum ada peringkat
- Form Accident ReportDokumen4 halamanForm Accident ReportKarthik SBelum ada peringkat
- PPE Matrix AgrocelDokumen2 halamanPPE Matrix AgrocelBhakti MahbubaniBelum ada peringkat
- Occupational Safety and Health Act (OSHA) 1994Dokumen69 halamanOccupational Safety and Health Act (OSHA) 1994WAN HAZIMBelum ada peringkat
- Formas 300 OSHA - 2004Dokumen3 halamanFormas 300 OSHA - 2004violet HumeBelum ada peringkat
- 9C - MSDS FiberglassDokumen3 halaman9C - MSDS FiberglassSon TranBelum ada peringkat
- PTW/Hot Work 2/checklist 34 - Excavations and Work WithinDokumen2 halamanPTW/Hot Work 2/checklist 34 - Excavations and Work WithinAli Shaikh AbdulBelum ada peringkat
- Family Emergency Contact PlanDokumen2 halamanFamily Emergency Contact PlanJeremy NashBelum ada peringkat
- BOMMI-PRD-03.0008-Rev.00 - Personal Protective EquipmentDokumen10 halamanBOMMI-PRD-03.0008-Rev.00 - Personal Protective Equipmentfundatia_gaudeamusBelum ada peringkat
- Fiberglass Cloth SdsDokumen5 halamanFiberglass Cloth Sdslance boxBelum ada peringkat
- TOPIC: Demolition SafetyDokumen1 halamanTOPIC: Demolition SafetyMohamed HamdallahBelum ada peringkat
- Caramics LotoDokumen7 halamanCaramics LotoAhmad MensaBelum ada peringkat
- DT-1 Cleaning PTWDokumen2 halamanDT-1 Cleaning PTWsubhashkpn86Belum ada peringkat
- Body MapDokumen1 halamanBody Mapapi-305532569Belum ada peringkat
- Hse Plan 2012Dokumen1 halamanHse Plan 2012Arief FirmansyahBelum ada peringkat
- Osha 3761Dokumen1 halamanOsha 3761api-301892310Belum ada peringkat
- GEN-021 Fact FindingDokumen3 halamanGEN-021 Fact Findingacanbasri1980Belum ada peringkat
- Risk Assessment CleaningDokumen7 halamanRisk Assessment Cleaningahmer09Belum ada peringkat
- Safety Alert - Danger of Infection - January 2010Dokumen1 halamanSafety Alert - Danger of Infection - January 2010Meklo1Belum ada peringkat
- Warehouse Risk Assessment Aldir II IWPPDokumen25 halamanWarehouse Risk Assessment Aldir II IWPPMadhu MohanBelum ada peringkat
- CL-07-02 Crane Lift Study ChecklistDokumen7 halamanCL-07-02 Crane Lift Study Checklisthanes0% (1)
- LO Procedure SampleDokumen6 halamanLO Procedure SampleNenad Spiki VukomanovicBelum ada peringkat
- Risk - Assessment - Form 14th Oct 2017Dokumen2 halamanRisk - Assessment - Form 14th Oct 2017hunstreteBelum ada peringkat
- Safety Alert Safety Alert: BackgroundDokumen1 halamanSafety Alert Safety Alert: BackgroundAnonymous h0yGTDQWZBelum ada peringkat
- Protect Yourself from Moving Machine PartsDokumen7 halamanProtect Yourself from Moving Machine PartsPedro ViegasBelum ada peringkat
- Toolbox Talks Working Around ExcavatorsDokumen2 halamanToolbox Talks Working Around ExcavatorspercyBelum ada peringkat
- New Osha300form1 1 04Dokumen3 halamanNew Osha300form1 1 04Anonymous YTiBI3P3tBelum ada peringkat
- Personal Protective EquipmentDokumen10 halamanPersonal Protective EquipmentXozanBelum ada peringkat
- Incident Investigation Report - Fire Incedent - 04-11-2018 Swati InteriorsDokumen4 halamanIncident Investigation Report - Fire Incedent - 04-11-2018 Swati InteriorsMobin Thomas AbrahamBelum ada peringkat
- Risk Assessment FormDokumen4 halamanRisk Assessment FormFrankie FryBelum ada peringkat
- Confined Space ENGDokumen30 halamanConfined Space ENGfaik395Belum ada peringkat
- Toolbox Talk 12 Banks Men Lifting GearDokumen2 halamanToolbox Talk 12 Banks Men Lifting GearSajid HussainBelum ada peringkat
- QA-IMCO-HSE-P-QT-015 Hot Work Procedure PDFDokumen16 halamanQA-IMCO-HSE-P-QT-015 Hot Work Procedure PDFFrancis Enriquez TanBelum ada peringkat
- Logout / Tagout Procedure Form: Equipment: Date Work Began: Work To Be ConductedDokumen1 halamanLogout / Tagout Procedure Form: Equipment: Date Work Began: Work To Be Conductedmanox007Belum ada peringkat
- SAFE520bP - Injury ReportDokumen1 halamanSAFE520bP - Injury ReportMiracle DavidBelum ada peringkat
- 01 - Safety - Introduction and Fundamental ConceptsDokumen32 halaman01 - Safety - Introduction and Fundamental Conceptsayman aydanBelum ada peringkat
- Sugeng Siswanto CV's May16Dokumen6 halamanSugeng Siswanto CV's May16Sitole S SiswantoBelum ada peringkat
- 1074 RT PH II Risk Assessment ERP - Template XLSX 01Dokumen109 halaman1074 RT PH II Risk Assessment ERP - Template XLSX 01aorukoBelum ada peringkat
- Road ReinstatementDokumen4 halamanRoad ReinstatementBishop Ojonuguwa AmehBelum ada peringkat
- Information Sheet About Safety in Welding MachineDokumen7 halamanInformation Sheet About Safety in Welding MachineMaryjoy VillajosBelum ada peringkat
- Project Monthly SHEQ Planning FormDokumen3 halamanProject Monthly SHEQ Planning FormParashuram PatilBelum ada peringkat
- OSHA Form 300 and 301 RecordsDokumen6 halamanOSHA Form 300 and 301 Recordsiese027Belum ada peringkat
- Osha 300 Log FormDokumen6 halamanOsha 300 Log FormJeff100% (1)
- 131 Single Width Fans DIMDokumen3 halaman131 Single Width Fans DIMJose Luis ChapasBelum ada peringkat
- Before You Design Inertial SeparatorDokumen4 halamanBefore You Design Inertial SeparatorbioarquitecturaBelum ada peringkat
- Pillars of Success1 PDFDokumen1 halamanPillars of Success1 PDFbioarquitecturaBelum ada peringkat
- Textbook BIOHDokumen48 halamanTextbook BIOHJavier CastroBelum ada peringkat
- E - 4 Engrapadoras (1) - ModelDokumen1 halamanE - 4 Engrapadoras (1) - ModelbioarquitecturaBelum ada peringkat
- 16 Axial 1000-2 Techo, 1200-4 (4) - ModelDokumen1 halaman16 Axial 1000-2 Techo, 1200-4 (4) - ModelbioarquitecturaBelum ada peringkat
- 5 Ways To Beat Back PainDokumen4 halaman5 Ways To Beat Back PainbioarquitecturaBelum ada peringkat
- Selecting Recir LS Pipe DiaDokumen24 halamanSelecting Recir LS Pipe DiaSiddharth JhambBelum ada peringkat
- Seventh SealDokumen34 halamanSeventh SealbioarquitecturaBelum ada peringkat
- Nep A GuidanceDokumen73 halamanNep A GuidancebioarquitecturaBelum ada peringkat
- The Master Plan For Planet Earth: Given by MaitreyaDokumen41 halamanThe Master Plan For Planet Earth: Given by MaitreyabioarquitecturaBelum ada peringkat
- Equipment Inventory DatabaseDokumen17 halamanEquipment Inventory DatabasebioarquitecturaBelum ada peringkat
- CO2 Evaporator Design Technical Bulletin PDFDokumen11 halamanCO2 Evaporator Design Technical Bulletin PDFbioarquitectura100% (1)
- Design 51 Backward InclinedDokumen4 halamanDesign 51 Backward InclinedbioarquitecturaBelum ada peringkat
- Jornada PDFDokumen5 halamanJornada PDFbioarquitecturaBelum ada peringkat
- Rockwell Current SolutionsDokumen45 halamanRockwell Current SolutionsbioarquitecturaBelum ada peringkat
- Overall LibreDokumen101 halamanOverall Librebioarquitectura50% (2)
- BoilerMACT HandbookDokumen64 halamanBoilerMACT HandbookbioarquitecturaBelum ada peringkat
- InformacioTecnica 02 SODECADokumen10 halamanInformacioTecnica 02 SODECAbioarquitecturaBelum ada peringkat
- PRINCIPLES OF RADIATION THERAPYDokumen11 halamanPRINCIPLES OF RADIATION THERAPYxxxbreadBelum ada peringkat
- TSF TechSpecs LSC22 T5 CRRTDokumen1 halamanTSF TechSpecs LSC22 T5 CRRTbioarquitecturaBelum ada peringkat
- RECIRCULATING LOOP CHILLER LOW PROFILE WEATHER-RESISTANTDokumen2 halamanRECIRCULATING LOOP CHILLER LOW PROFILE WEATHER-RESISTANTbioarquitecturaBelum ada peringkat
- Civ Co Source BookDokumen106 halamanCiv Co Source BookbioarquitecturaBelum ada peringkat
- Fire Safety Risk Management - Module ThreeDokumen16 halamanFire Safety Risk Management - Module Threeg5nbBelum ada peringkat
- Construction Fundamental Study GuideDokumen82 halamanConstruction Fundamental Study GuidebryanshaoBelum ada peringkat
- REVISED Arlington 360 - Apartments Multi - Project - RFP 11.08.23Dokumen23 halamanREVISED Arlington 360 - Apartments Multi - Project - RFP 11.08.23Siddharth SasidharanBelum ada peringkat
- 1 Pengenalan OshDokumen29 halaman1 Pengenalan OshMohdhafizFaiz MdAliBelum ada peringkat
- Moving Rotating EquipmentDokumen35 halamanMoving Rotating EquipmentAun AbbasBelum ada peringkat
- Qualification Procedure No. 2: SSPC: The Society For Protective CoatingsDokumen11 halamanQualification Procedure No. 2: SSPC: The Society For Protective CoatingsanoopkumarBelum ada peringkat
- History of Public HealthDokumen38 halamanHistory of Public HealthEdgar DumagpiBelum ada peringkat
- Lesson 124Dokumen5 halamanLesson 124jerimiah_manzonBelum ada peringkat
- Guide To Selecting Fixed vs. Portable Gas Detection DevicesDokumen29 halamanGuide To Selecting Fixed vs. Portable Gas Detection Devicesdelta_scopeBelum ada peringkat
- Chris Rainwater CV 2013Dokumen7 halamanChris Rainwater CV 2013api-235273771Belum ada peringkat
- Achieve ZERO Final For PrintingDokumen138 halamanAchieve ZERO Final For Printingj brotherBelum ada peringkat
- LEGAL AND ETHICAL ISSUES IN CHEMICAL AND BIOPROCESS INDUSTRIESDokumen102 halamanLEGAL AND ETHICAL ISSUES IN CHEMICAL AND BIOPROCESS INDUSTRIESAmirul AdeebBelum ada peringkat
- Warning! Behavior-Based Safety Can Be Hazardous To Your Health and Safety Program!Dokumen24 halamanWarning! Behavior-Based Safety Can Be Hazardous To Your Health and Safety Program!HevyBelum ada peringkat
- OHAS Midterm Quiz 1 - Attempt ReviewDokumen7 halamanOHAS Midterm Quiz 1 - Attempt ReviewNot Racist By The WayBelum ada peringkat
- MSDS Full1Dokumen92 halamanMSDS Full1Sunthron SomchaiBelum ada peringkat
- 37-2013-00078268-Cu-Bt-Ctl Roa-1 12-04-13 Complaint 1386637937306Dokumen118 halaman37-2013-00078268-Cu-Bt-Ctl Roa-1 12-04-13 Complaint 1386637937306api-218643948Belum ada peringkat
- Builder Mag Q124Dokumen68 halamanBuilder Mag Q124Gary McKayBelum ada peringkat
- Silica Sand MSDSDokumen9 halamanSilica Sand MSDSecoscribdBelum ada peringkat
- 2015 Maintenance Department Meeting HighlightsDokumen34 halaman2015 Maintenance Department Meeting HighlightsRemy AhmadBelum ada peringkat