IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 6 Ver. II (Jun. 2015), PP 25-28
www.iosrjournals.org
Richters Type Femoral Hernia: Diagnostic Difficulty
Dr. J Janardhan1, Dr. K Sreedhar Rao2, Dr. P Venkateswar3,
Dr. K Deepthi4, Dr B Bhavya5
1
Assistant Professor, Department of General Surgery, Osmania Medical College & Hospital, Hyderabad.
Professor, Department of General Surgery, Osmania Medical College & Hospital, Hyderabad.
3
Associate Professor, Department of General Surgery, Osmania Medical College & Hospital, Hyderabad.
4, 5
Post Graduate Student, Department of General Surgery, Osmania Medical College & Hospital, Hyderabad.
2
Abstract: Femoral hernias are relatively uncommon; however, they are the most common incarcerated
abdominal hernias with strangulation of viscous carrying significant mortality. Femoral hernia has often been
found to be the cause of unexplained bowel obstruction. Femoral hernias are known for atypical presentations
like painless groin swelling, groin cellulitis/necrotizing fasciitis. Diagnosing Richters femoral hernia is often
difficult especially in obese patients. Delay in diagnosis may occur, especially because a strangulated femoral
hernia doesnt always present with typical groin swelling and signs of strangulation. We report a case of 58 yr
old female presenting with abdominal distension and vomiting since 15days, with a non tender swelling in right
groin without signs of strangulation. On exploration, Richters femoral hernia with part of small bowel wall as
content which was gangrenous necessitating resection and anastomosis.
Keywords: Richters femoral hernia, Strangulation, Groin swelling.
I. Introduction
The earliest known reported case of Richters hernia occurred in 1598 and was described by Fabricius
Hildanus. The first scientific description of this particular hernia was given by August Gottlob Richter in 1778,
who presented it as the small rupture. In 1887, Sir Frederick Treves gave an excellent overview on the topic
and proposed the title Richters hernia. To his worka cornerstone to modern understandinghardly any
new aspects can be added today. Since then, only occasional case reports or small series of retrospectively
collected Richters hernias have been published [1].
Femoral hernia is relatively uncommon, making up 2-8% of all adult groin hernias. Incarcerated
femoral hernias, however, are most common incarcerated abdominal hernias with strangulation of viscous
carrying up to 14% mortality. They have high rate of complications owing to narrowness and rigidity of femoral
canal. It is twice common in parous women than nonparous women. Approximately 60% of femoral hernias are
found on right side, 30% in left side and 10% are bilateral. They typically present as a groin lump clinically
lateral and inferior to pubic tubercle. They often require emergency surgery because of incarceration or
strangulation of intestine. In addition, intestinal resection may need to be considered based on intestinal
viability.
Factors predisposing to femoral hernias include pregnancy, obesity, pelvic mass, urinary retention and
constipation. Furthermore, weakening of transversalis fascia due to old age may be implicated. Diagnosing the
lump in groin is often difficult especially in obese patients. Delay in diagnosis may occur, especially because a
strangulated femoral hernia doesnt always typically present with groin swelling and local signs of strangulation.
Differential diagnosis of femoral hernia includes pseudohernia, Femoral artery pseudoaneurysm,
Saphenous vein varicosity, Soft tissue masses and lymphadenopathy which can be differentiated by proper
clinical examination and imaging. Definitive preoperative diagnosis and strategic planning for surgery are thus
important as it can be easily mistaken with other differential diagnosis of groin swellings and most importantly
it doesnt always present with typical features of strangulation as in our case.
II.
Case Report
A 58 yr old female presented with abdominal distension, vomitings since 15 days and constipation
since 5 days. History of present illness started as diffuse pain abdomen, vomiting [bilious and undigested food].
No fever, no past surgeries. On examination she was apyrexic, PR: 100/min, BP: 110/70, RR: 16/min, a non
tender, irreducible, mobile 3x3cm swelling found in the right groin with no signs of inflammation/strangulation
[Fig-1]. Abdomen distended but soft, no tenderness and absent bowel sounds.
Work up in the emergency department showed unremarkable blood investigations, X-ray erect
abdomen showed distended bowel loops with multiple air fluid levels, USG & CT abdomen were reported as
small bowel obstruction probably at terminal ileum with collapsed large bowel loops & A single enlarged right
inguinal lymphnode . Later a repeat USG by an experienced radiologist revealed the suspicion of right femoral
DOI: 10.9790/0853-14622528
www.iosrjournals.org
25 | Page
Richters Type Femoral Hernia: Diagnostic Difficulty
hernia with bowel incarceration. The patient was subsequently taken to the theatre and right inguinal region
explored with transinguinal approach which confirmed a right sided Richters femoral hernia with part of the
small bowel wall as content which was gangrenous and opened up [Fig-2&3]. Inguinal ligament was divided in
this case to release the neck of the sac [Fig-4]. Resection of gangrenous segment and end to end anastomosis
was done in two layers. Posterior wall repaired with reinforcement of inguinal ligament to the pectineal ligament
using interrupted non absorbable sutures (20 prolene). Mesh was avoided due to gross contamination of
wound, gangrenous bowel and delayed presentation. Post operative period was uneventful and she was
discharged on POD 10.
III. Discussion
The precondition for the formation of this particular hernia, as stated by Richter, is determined by the
size and consistency of the hernial orifice: it must be big enough to ensnare the bowel wall, but small enough to
prevent protrusion of an entire loop of the intestine, and the margin of the hernial ring must be firm [6].
According to others the presence of a tight constricting ring is a prerequisite for strangulation and compromised
blood circulation, which finally leads to ischemia and gangrene [7, 8]. Richters hernias tend to progress more
rapidly to gangrene than ordinary strangulated ones This may be explained not only by the firm constricting ring
that exerts direct pressure on the bowel wall, but also by the anatomical peculiarity that, as a rule, it is the free
border of the intestine opposite the mesentery with the predominance of terminal arterioles that is involved. It
can also be explained by the time factor. In most cases, where less than two thirds of the circumference of the
bowel wall is involved [Fig-5], the lumen of the gut remains free and an alarming intestinal obstruction is
absent. This insidious pathologic feature of Richters hernia often leads to late diagnosis or even misdiagnosis,
thus allowing time for bowel necrosis to develop.
Making the diagnosis of Richters hernia may be difficult because of the apparently innocuous initial
symptoms and sparse clinical findings; the diagnosis may remain presumptive until clearly confirmed at surgery.
The first mild symptoms, such as vague abdominal pain and slight malaise, may not be appreciated, resulting in
delayed diagnosis [7,8]. There may be nausea and vomiting, but they are on the whole less common and less
severe than in the usual form of strangulation because obstruction is rarely complete. Clinical and radiologic
signs of an ileus are present in approximately 10% of patients; in the absence of a complete mechanical
obstruction, this can be due to paralysis. Local signs may be absent or discrete and, if present, are easily
overlooked or misinterpreted. Throughout the literature, the most constant physical finding remains tenderness
or swelling over a potential hernial orifice. Overlying erythema should heighten the index of suspicion.
A small hernia in the femoral canal, the most common site of Richters hernia (in whites), is sometimes
masked by body fat or an enlarged lymph node or is mistaken for acute lymphadenitis. If local gangrene of the
intestinal wall occurs, the classic signs of inflammation appear (painful swelling, redness of the overlying skin,
and local heat). In the early stage, this groin swelling can be discrete and can appear as a local abscess or as
subcutaneous emphysema caused by anaerobic infection.
If surgery is performed too late or not at all, natural healing may occur in the form of drainage through
an enterocutaneous fistula. Under certain conditions (a self-limiting septic process, a low-output fistula, and
free intestinal passage), the fistula may spontaneously close, as observed by Fabricius Hildanus, but it may also
persist for months, as reported by others [11, 12]. Perforation into another compartment, such as the scrotum,
vulva, thighs, or peritoneal cavity [13], may also occur, producing a severe clinical course with considerable
morbidity and a high death rate. With the appearance of peritonitis, the prognosis becomes highly unfavorable.
Gangrene has been found as early as the third day of strangulation [10], but the development of an
enterocutaneous fistula may take as long as several months
Patients with perforated hernia require timely and sometimes aggressive preoperative resuscitation,
consisting of isotonic rehydration and antibiotic therapy. In some cases, positive preoperative balances up to
9,000 ml were necessary. Surgery is the only treatment. Richters hernias in the groin without apparent signs of
perforation can be handled as ordinary inguinal hernias. Preliminary attempts at manual reduction should be
avoided because the viability of the hernial sac can be determined by direct inspection only. When possible, we
avoid a segmental resection and close the defect after a careful debridement of the margins. However, the rule
regarding strangulation (When in doubt, resect) should be respected.
Classically three approaches are described to open femoral hernia repair: Lockwood's infra-inguinal,
Lotheissen's trans-inguinal and McEvedy's high approach. Irrespective of the approach used the following will
be achieved: Dissection of sac, Reduction/inspection of contents, Resection if the bowel is nonviable, ligation of
sac and approximation of inguinal and pectineal ligaments. In our case we used a transingunal approach for
femoral canal [Fig.6].
DOI: 10.9790/0853-14622528
www.iosrjournals.org
26 | Page
Richters Type Femoral Hernia: Diagnostic Difficulty
IV. Figures
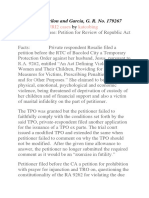
Fig-1: Pre operative groin swelling with no skin
changes
Fig-2: Femoral hernia below inguinal ligament
Fig-3 : Gangrenous & opened up small bowel
content
Fig-5: Partial entrapment of bowel wall
with preservation of luminal continuity.
DOI: 10.9790/0853-14622528
Fig-4 : Division of inguinal ligament
to release the neck
Fig-6 : Transinguinal approach-post operative
scar photo.
www.iosrjournals.org
27 | Page
Richters Type Femoral Hernia: Diagnostic Difficulty
V. Conclusion
Femoral hernia has often been found to be the cause of unexplained bowel obstruction. An abdominal
X-ray showing small bowel obstruction in a female patient with painful groin lump needs no further
investigation. Diagnosis is largely a clinical one. However, in difficult patients as in obese, imaging in the form
of USG abdomen & CT/MRI may help in diagnosis. The entrapped small segment of bowel wall would be
difficult to visualize on computed tomography, and contrast studies would be unrevealing in the early stages,
when there is still patency. Therefore, awareness during the clinical examination remains the key for proper
diagnosis and timely surgery.
Correct preoperative diagnosis of femoral hernia and strict operative strategy are of utmost importance
to prevent undue morbidity and mortality. Once the diagnosis is established, the acute infection phase is under
control, and the patient undergoes successful surgery, the outcome does not differ from that of ordinary
strangulated hernias.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
Ann Surg. 2000 Nov; 232(5): 710718. PMCID: PMC1421226
Davd T:Strangulated femoral hernia, Med J Aust 1967,1:258.
Franklin ME etal,Preliminary experience with new bioactive prosthetic material for repair of infective fields, hernia pubmed
2002,601-6, 171-174.
Tingwald GR, Cooperman M,Inguinal and Femoral hernia repair in geriatric patients, Surg Gynaec Obst 1982, 154:704-706.
Kulah B etal, Emergency hernia repairs in elderly patients, Am J Surg 2001, 182(5),455-459.
Richter AG. Abhandlung von den Brchen. Gttingen: Johann Christian Dieterich; 1785.
Pualwuan F. Operative aspects of Richters hernia. Surg Gynecol Obstet 1958;106:358 362. [PubMed]
Keynes WM. Richters hernia. Surg Gynecol Obstet 1956; 103: 496500. [PubMed]
O MC.Donnell, A Adas, An obstructed femoral hernia, the internet journal of radiology, vol.7,no.1, 2006.
Treves F. Richters hernia or partial enterocele. Med Chir Tr 1887; 17: 149167. [PMC free article][PubMed]
Udofot SU. Multiple fecal and urinary fistulae as a complication of native treatment of inguinal hernia. Trop Geogr Med 1990; 43:
105. [PubMed]
Fckiger R, Huber A. Die Richtersche Hernie. Der Chirurg 1993; 64: 822826. [PubMed]
Limjoco UR, Grubbs JM, Thomas MD. Richters hernia with bowel perforation. Am Fam Physician 1998; 58: 352354. [PubMed]
DOI: 10.9790/0853-14622528
www.iosrjournals.org
28 | Page
Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- String Harmonics in Ravel's Orchestral WorksDokumen97 halamanString Harmonics in Ravel's Orchestral WorksYork R83% (6)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Kinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationDokumen6 halamanKinesics, Haptics and Proxemics: Aspects of Non - Verbal CommunicationInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Bagpipe Student Manual PDFDokumen116 halamanBagpipe Student Manual PDFRhonda Seiter75% (4)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Human Rights and Dalits: Different Strands in The DiscourseDokumen5 halamanHuman Rights and Dalits: Different Strands in The DiscourseInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Garcia vs. J. Drilon G. R. No. 179267 Case DigestDokumen5 halamanGarcia vs. J. Drilon G. R. No. 179267 Case DigestJoannMarieBrenda delaGenteBelum ada peringkat
- GDPR in ChartsDokumen13 halamanGDPR in ChartsImageking0% (2)
- The Impact of Technologies On Society: A ReviewDokumen5 halamanThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- Fitch CLOs and Corporate CDOsRating Criteria PDFDokumen57 halamanFitch CLOs and Corporate CDOsRating Criteria PDFantonyBelum ada peringkat
- AripiprazoleDokumen2 halamanAripiprazoleKrisianne Mae Lorenzo FranciscoBelum ada peringkat
- LL - Farsi IntroductionDokumen13 halamanLL - Farsi IntroductionPiano Aquieu100% (1)
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDokumen5 halamanAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDokumen5 halaman"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDokumen6 halamanThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDokumen7 halamanSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDokumen7 halamanA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDokumen14 halamanAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Assessment of The Implementation of Federal Character in Nigeria.Dokumen5 halamanAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Belum ada peringkat
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDokumen5 halamanEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Dokumen15 halamanA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Belum ada peringkat
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDokumen7 halamanComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDokumen4 halamanInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDokumen5 halamanRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDokumen7 halamanTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- The Lute Against Doping in SportDokumen5 halamanThe Lute Against Doping in SportInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDokumen5 halamanDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalBelum ada peringkat
- Importance of Mass Media in Communicating Health Messages: An AnalysisDokumen6 halamanImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Transforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweDokumen9 halamanTransforming People's Livelihoods Through Land Reform in A1 Resettlement Areas in Goromonzi District in ZimbabweInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Role of Madarsa Education in Empowerment of Muslims in IndiaDokumen6 halamanRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Beowulf: A Folktale and History of Anglo-Saxon Life and CivilizationDokumen3 halamanBeowulf: A Folktale and History of Anglo-Saxon Life and CivilizationInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Motivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweDokumen8 halamanMotivational Factors Influencing Littering in Harare's Central Business District (CBD), ZimbabweInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Classical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahDokumen9 halamanClassical Malay's Anthropomorphemic Metaphors in Essay of Hikajat AbdullahInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Women Empowerment Through Open and Distance Learning in ZimbabweDokumen8 halamanWomen Empowerment Through Open and Distance Learning in ZimbabweInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- An Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsDokumen6 halamanAn Exploration On The Relationship Among Learners' Autonomy, Language Learning Strategies and Big-Five Personality TraitsInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Substance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaDokumen11 halamanSubstance Use and Abuse Among Offenders Under Probation Supervision in Limuru Probation Station, KenyaInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Micro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaDokumen3 halamanMicro Finance and Women - A Case Study of Villages Around Alibaug, District-Raigad, Maharashtra, IndiaInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Design Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextDokumen6 halamanDesign Management, A Business Tools' Package of Corporate Organizations: Bangladesh ContextInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- A Study On The Television Programmes Popularity Among Chennai Urban WomenDokumen7 halamanA Study On The Television Programmes Popularity Among Chennai Urban WomenInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- At HomeDokumen16 halamanAt HomesamoorewritesBelum ada peringkat
- CSE 191 Homework Proposition LogicDokumen5 halamanCSE 191 Homework Proposition LogicJyothi AnkumBelum ada peringkat
- Sidak 2008 FAQsDokumen3 halamanSidak 2008 FAQssikhswimBelum ada peringkat
- Speaking EMN4Dokumen61 halamanSpeaking EMN4Khánh LinhBelum ada peringkat
- Physics: PAPER 1 Multiple ChoiceDokumen20 halamanPhysics: PAPER 1 Multiple Choicelulz.l.n.sBelum ada peringkat
- SAP Training Program Proposal for StudentsDokumen2 halamanSAP Training Program Proposal for StudentsAjay KumarBelum ada peringkat
- BuddhismDokumen49 halamanBuddhismFabio NegroniBelum ada peringkat
- Unit 1 DinosaurDokumen5 halamanUnit 1 DinosaurAnamika ShabnamBelum ada peringkat
- 2 10 1 PBDokumen4 halaman2 10 1 PBHeesung KimBelum ada peringkat
- ELC650-Movie Critique Yusri, YassinDokumen14 halamanELC650-Movie Critique Yusri, YassinYusri MalekBelum ada peringkat
- Francis Asbury Revival Study PDFDokumen10 halamanFrancis Asbury Revival Study PDFLauRa Segura VerasteguiBelum ada peringkat
- Sigram Schindler Beteiligungsgesellschaft PetitionDokumen190 halamanSigram Schindler Beteiligungsgesellschaft PetitionjoshblackmanBelum ada peringkat
- DTF - Houses of The FallenDokumen226 halamanDTF - Houses of The FallenShuang Song100% (1)
- Chapter 8Dokumen3 halamanChapter 8sasafoadjeiBelum ada peringkat
- A History Analysis and Performance Guide To Samuel Barber?Dokumen117 halamanA History Analysis and Performance Guide To Samuel Barber?giorgio planesioBelum ada peringkat
- Hbo Group AnalysisDokumen5 halamanHbo Group AnalysisAlexa Dei GalinatoBelum ada peringkat
- NSTP 2 Modules Lesson on Community OrganizingDokumen14 halamanNSTP 2 Modules Lesson on Community OrganizingJestony Riray CagmatBelum ada peringkat
- Tango With DjangoDokumen191 halamanTango With DjangoZachary JamesBelum ada peringkat
- Di Bella Et Al 2004Dokumen13 halamanDi Bella Et Al 2004Emilio Patané SpataroBelum ada peringkat
- LESSON 1.1.2 - Online PlatformsDokumen5 halamanLESSON 1.1.2 - Online PlatformsAndree Laxamana100% (1)
- Gauteng Grade 6 Maths ExamDokumen14 halamanGauteng Grade 6 Maths ExamMolemo S MasemulaBelum ada peringkat
- Agenda For Regular Board Meeting February 18, 2022 Western Visayas Cacao Agriculture CooperativeDokumen2 halamanAgenda For Regular Board Meeting February 18, 2022 Western Visayas Cacao Agriculture CooperativeGem Bhrian IgnacioBelum ada peringkat