Anda mungkin juga menyukai
- Transverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesDari EverandTransverse Myelitis, A Simple Guide To The Condition, Treatment And Related DiseasesPenilaian: 5 dari 5 bintang5/5 (1)
- 1 - Skeletal Muscle DisordersDokumen32 halaman1 - Skeletal Muscle DisordersGarrett ZajicekBelum ada peringkat
- 08.01.24 Dr. Helal, DMD, CPD-2Dokumen60 halaman08.01.24 Dr. Helal, DMD, CPD-2Minhajul IslamBelum ada peringkat
- Muscle Disease For PhysiosDokumen46 halamanMuscle Disease For PhysiosKrishna KanthBelum ada peringkat
- Neuromuscular dis د.رشاد عبدالغنيDokumen47 halamanNeuromuscular dis د.رشاد عبدالغنيMohammad Belbahaith100% (1)
- Mod9Week7 - PA 3306 - Oct 2&3Dokumen64 halamanMod9Week7 - PA 3306 - Oct 2&3komal sheikhBelum ada peringkat
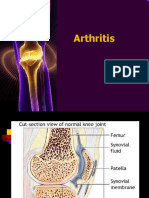
- Arthritis 180325095830 PDFDokumen77 halamanArthritis 180325095830 PDFHesoca HuxBelum ada peringkat
- Als Med Surg Group 2Dokumen17 halamanAls Med Surg Group 2David MharkBelum ada peringkat
- Skeletal Muscle Pathology For Second Year Dental Students: by Dr. Ioannis G. KoutlasDokumen8 halamanSkeletal Muscle Pathology For Second Year Dental Students: by Dr. Ioannis G. KoutlasnaglaramdanBelum ada peringkat
- Disorders of Skeletal MuscleDokumen31 halamanDisorders of Skeletal Muscleapi-19916399Belum ada peringkat
- Myopathy: By: Rey MartinoDokumen16 halamanMyopathy: By: Rey Martinorey martinoBelum ada peringkat
- Systematic PathologyDokumen119 halamanSystematic Pathologypatricemuza69Belum ada peringkat
- 22 Disorders of Skeletal Muscle by DR NazishDokumen41 halaman22 Disorders of Skeletal Muscle by DR NazishAhmed YTBelum ada peringkat
- Kelainan Neuromuskuler: Dr. Luhu A. Tapiheru, SP.S Fakultas Kedokteran Universitas Muhammadiyah MedanDokumen84 halamanKelainan Neuromuskuler: Dr. Luhu A. Tapiheru, SP.S Fakultas Kedokteran Universitas Muhammadiyah MedandanieliqbalBelum ada peringkat
- Diseases of The MuscleDokumen51 halamanDiseases of The MuscleGianina RafaelBelum ada peringkat
- Cell and Tissue InjuryDokumen60 halamanCell and Tissue InjurydesiBelum ada peringkat
- Approach To Myopathy by AnkitDokumen83 halamanApproach To Myopathy by AnkitankitBelum ada peringkat
- CBT Ortho 1Dokumen45 halamanCBT Ortho 1putri umepalBelum ada peringkat
- Pathology Muskulo SkletalDokumen68 halamanPathology Muskulo SkletalwilliamBelum ada peringkat
- Muscular Dystrophy NoteDokumen6 halamanMuscular Dystrophy NoteMd. Sherajul HaqueBelum ada peringkat
- Osteoartritis Dan GoutDokumen66 halamanOsteoartritis Dan GoutReioctabianoBelum ada peringkat
- Disturbances of Growth Asnan Sphinx 6 PDFDokumen20 halamanDisturbances of Growth Asnan Sphinx 6 PDFmina hishamBelum ada peringkat
- 7 Soft Tissue Tumor-Muscular DystrophyDokumen23 halaman7 Soft Tissue Tumor-Muscular DystrophyDikpal BikramBelum ada peringkat
- Classification of Disorders of Musculoskeletal System (MSK) : Presented By: Siti Sarah Maha Dewi Bong Jen NeeDokumen69 halamanClassification of Disorders of Musculoskeletal System (MSK) : Presented By: Siti Sarah Maha Dewi Bong Jen NeeBONG AIKCHINGBelum ada peringkat
- Assesment Rheumatoid ArthritisDokumen39 halamanAssesment Rheumatoid ArthritisKlinik SakuramedicaBelum ada peringkat
- FinalDokumen87 halamanFinalSanjiv GoyalBelum ada peringkat
- Biochemistry-Musculoskeletal DisorderDokumen17 halamanBiochemistry-Musculoskeletal DisorderSyifa SalsabilaBelum ada peringkat
- Pathology Lecture SeriesDokumen168 halamanPathology Lecture SeriesButch DumdumBelum ada peringkat
- Epidemiology, Genetics, PathophysiologyDokumen18 halamanEpidemiology, Genetics, PathophysiologySutapa PawarBelum ada peringkat
- Osteoarthritis (Oa) : Prakash Thakulla InternDokumen48 halamanOsteoarthritis (Oa) : Prakash Thakulla InternPrakash ThakullaBelum ada peringkat
- Bone Disorders PPT Part 4 of 4Dokumen28 halamanBone Disorders PPT Part 4 of 4Mister CrabsBelum ada peringkat
- NewGeneral Pathology2Dokumen305 halamanNewGeneral Pathology2Tahir AzizBelum ada peringkat
- (K25) Path - Musculosceletal FK Part 2Dokumen69 halaman(K25) Path - Musculosceletal FK Part 2Virginia JawaBelum ada peringkat
- Complications of FractureDokumen19 halamanComplications of FractureEsome Sharma100% (1)
- JointsDokumen68 halamanJointsLaine ZeeBelum ada peringkat
- MyopathyDokumen47 halamanMyopathySOUMYADEEP BHUINYABelum ada peringkat
- Rheumatology: Osteoarthritis Rheumatoid Arthritis: Dr. Meg-Angela Christi AmoresDokumen25 halamanRheumatology: Osteoarthritis Rheumatoid Arthritis: Dr. Meg-Angela Christi AmoresNinaBelum ada peringkat
- OSTEOARTHRITISDokumen29 halamanOSTEOARTHRITISValabhoju Bindu MadhaviBelum ada peringkat
- NewGeneral Pathology2Dokumen305 halamanNewGeneral Pathology2Tahir AzizBelum ada peringkat
- Cell InjuryDokumen132 halamanCell InjuryAboubakar Moalim Mahad moh'dBelum ada peringkat
- Polymyositis DermatomyositisDokumen2 halamanPolymyositis DermatomyositisTay Woo ChiaoBelum ada peringkat
- MuscolskeletalDokumen74 halamanMuscolskeletalsamar yousif mohamedBelum ada peringkat
- 病理國考複習 PDFDokumen61 halaman病理國考複習 PDFAnonymous ZUQcbcBelum ada peringkat
- Cellular Responses To Stress and Toxic Insults: Adaptation, Injury, and DeathDokumen26 halamanCellular Responses To Stress and Toxic Insults: Adaptation, Injury, and DeathHusam ShawaqfehBelum ada peringkat
- Screenshot 2022-11-29 at 1.52.52 PMDokumen13 halamanScreenshot 2022-11-29 at 1.52.52 PMf267wbmdfkBelum ada peringkat
- Common Bone Disorders: Bone and Cartilage Deterioration Is A Natural Process As We AgeDokumen28 halamanCommon Bone Disorders: Bone and Cartilage Deterioration Is A Natural Process As We Ageluckyswiss7776848Belum ada peringkat
- Myopathy: Continuing Education ActivityDokumen15 halamanMyopathy: Continuing Education ActivityHerry GunawanBelum ada peringkat
- Myotonic Dystrophy Type I (Steinert's Disease)Dokumen3 halamanMyotonic Dystrophy Type I (Steinert's Disease)Mohan KrishabiBelum ada peringkat
- Collagen Presentation 2Dokumen8 halamanCollagen Presentation 2Sanjay VeerasammyBelum ada peringkat
- Myopathies: Presenter: DR Edom G/medhin (IMR3) Moderator: DR Teklil Hagos (Consultant Neurologist) July 23 /2021Dokumen48 halamanMyopathies: Presenter: DR Edom G/medhin (IMR3) Moderator: DR Teklil Hagos (Consultant Neurologist) July 23 /2021Meseret Hamer ZewdieBelum ada peringkat
- Anaphy Lec DiseaseDokumen8 halamanAnaphy Lec DiseaseJules ConcepcionBelum ada peringkat
- OsteoarthritisDokumen40 halamanOsteoarthritiskylieverBelum ada peringkat
- Osteogenesis Imperfecta, AMCDokumen6 halamanOsteogenesis Imperfecta, AMCmakananlezatBelum ada peringkat
- Class 2Dokumen65 halamanClass 2hari dharshanBelum ada peringkat
- Osteomyelitis: Pediatric Surgery Department Andreev D.ADokumen83 halamanOsteomyelitis: Pediatric Surgery Department Andreev D.AlimeddyBelum ada peringkat
- IT 1 Introduction Blok 22 - PRMDokumen18 halamanIT 1 Introduction Blok 22 - PRMApriyani Supia DewiBelum ada peringkat
- UU 5 1997psikotropikaDokumen85 halamanUU 5 1997psikotropikaMeilina PutriBelum ada peringkat
- Muscular DystrophiesDokumen36 halamanMuscular DystrophiesAbdullah AzamBelum ada peringkat
- 2011 Spring SURGERY III BY Ismail Answere: Past Papers Question andDokumen11 halaman2011 Spring SURGERY III BY Ismail Answere: Past Papers Question andDerranMorganBelum ada peringkat
- Necrosis and Cellualr AdaptationDokumen56 halamanNecrosis and Cellualr AdaptationEs SarveshBelum ada peringkat
- Book PDFDokumen186 halamanBook PDFLuis CcenchoBelum ada peringkat
- Obstetric by 10 Teachers Chapter 8Dokumen25 halamanObstetric by 10 Teachers Chapter 8FerasBelum ada peringkat
- Hirschsprung Disease (Congenital Aganglionic Megacolon) : PathophysiologyDokumen2 halamanHirschsprung Disease (Congenital Aganglionic Megacolon) : PathophysiologyDiane Mary S. Mamenta100% (1)
- Dilation and CurettageDokumen2 halamanDilation and CurettageElisse GarciaBelum ada peringkat
- JSS MoUDokumen88 halamanJSS MoUchetanhiremathBelum ada peringkat
- Corticosteroids 24613Dokumen33 halamanCorticosteroids 24613NOorulain HyderBelum ada peringkat
- TumorDokumen8 halamanTumorputyCeria86Belum ada peringkat
- Malaika Nakupenda MalaikaDokumen11 halamanMalaika Nakupenda MalaikaMuhidin Issa MichuziBelum ada peringkat
- 1-History of Surgery in UkraineDokumen16 halaman1-History of Surgery in UkraineErdemBelum ada peringkat
- Exercises in Epidemiology Applying Principles and MethodsDokumen266 halamanExercises in Epidemiology Applying Principles and MethodsVivin Fitriana91% (11)
- Test ExpositionDokumen9 halamanTest ExpositionFatimatuz Zahro'Belum ada peringkat
- THORACENTESISDokumen9 halamanTHORACENTESISJohn Ray J. PaigBelum ada peringkat
- Pemeriksaan Colok DuburDokumen9 halamanPemeriksaan Colok DuburRidwan Hadinata SalimBelum ada peringkat
- Approach To Patients EULARDokumen35 halamanApproach To Patients EULARstuckinbedBelum ada peringkat
- Physiology of The PancreasDokumen4 halamanPhysiology of The PancreasClayton VerBerkmösBelum ada peringkat
- Multidisciplinary Patient Care Navigator To Help Patients at Brinton Lake - Crozer-Keystone Health System - PADokumen2 halamanMultidisciplinary Patient Care Navigator To Help Patients at Brinton Lake - Crozer-Keystone Health System - PAnbmyersBelum ada peringkat
- Giant Cell Lesions of The Jaws: DR Syeda Noureen IqbalDokumen61 halamanGiant Cell Lesions of The Jaws: DR Syeda Noureen IqbalMuhammad maaz khanBelum ada peringkat
- Arab Board Final 2018 - 2Dokumen12 halamanArab Board Final 2018 - 2lonsilord17Belum ada peringkat
- Malignancy Yield of Testis PathologyDokumen7 halamanMalignancy Yield of Testis PathologyadolfoBelum ada peringkat
- Total Glossectomy For Tongue CancerDokumen10 halamanTotal Glossectomy For Tongue CancerRajan KarmakarBelum ada peringkat
- PTW PresentationDokumen44 halamanPTW PresentationGina RBelum ada peringkat
- Telus Health - Care Centres Elite Preventative Health Assessment 2021Dokumen2 halamanTelus Health - Care Centres Elite Preventative Health Assessment 2021sergii volodarskiBelum ada peringkat
- Revised Proposal Water TreatmentDokumen13 halamanRevised Proposal Water TreatmentBryan Henson CarreonBelum ada peringkat
- Airway Management - DR Dedi SpAnDokumen120 halamanAirway Management - DR Dedi SpAnBagus Abdillah WinataBelum ada peringkat
- Tawam Gen InfoDokumen10 halamanTawam Gen InfoiknowvskiBelum ada peringkat
- Drug Use During Pregnancy and LactationDokumen50 halamanDrug Use During Pregnancy and LactationJuveria Fatima75% (4)
- Power Guard 818 MSDSDokumen4 halamanPower Guard 818 MSDSPowerGuardSealersBelum ada peringkat
- Creatine Kinase. by AsifDokumen10 halamanCreatine Kinase. by AsifharisBelum ada peringkat
- Kardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313Dokumen2 halamanKardex: Diet: Interventions IVF (Indicate Date and Time Started) Room Number: 313kuro hanabusaBelum ada peringkat
- (23933356 - Romanian Journal of Rhinology) Sphenoid Rhinosinusitis Associated With Abducens Nerve Palsy - Case ReportDokumen6 halaman(23933356 - Romanian Journal of Rhinology) Sphenoid Rhinosinusitis Associated With Abducens Nerve Palsy - Case ReportFoppy PuspitasariBelum ada peringkat