Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (120)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- July2005 Vitamin Research NewsDokumen16 halamanJuly2005 Vitamin Research Newsullikeit100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Little Book of Pediatrics PDFDokumen208 halamanThe Little Book of Pediatrics PDFPaulo GouveiaBelum ada peringkat
- ATLS ProtocoloDokumen21 halamanATLS Protocoloedgarjavier65100% (2)
- Delayed Vs Immediate Umbilical Cord ClampingDokumen37 halamanDelayed Vs Immediate Umbilical Cord ClampingAndi DeviriyantiBelum ada peringkat
- Testicular CancerDokumen24 halamanTesticular CancerJulianne LeeBelum ada peringkat
- Lesson Plan On Minor Disorders During Pregnancy Its Management 1Dokumen20 halamanLesson Plan On Minor Disorders During Pregnancy Its Management 1Bhawna Joshi100% (6)
- Antenatal Care: Muhammad Wasil Khan and Ramsha MazharDokumen55 halamanAntenatal Care: Muhammad Wasil Khan and Ramsha MazharmarviBelum ada peringkat
- Pato GenesisDokumen3 halamanPato GenesisDwi LestariBelum ada peringkat
- English Task: Name: Indah Aqilah Febriani Class: 8.2Dokumen4 halamanEnglish Task: Name: Indah Aqilah Febriani Class: 8.2Dwi LestariBelum ada peringkat
- Status Coass 14 HalDokumen18 halamanStatus Coass 14 HalDwi LestariBelum ada peringkat
- Chapter 196Dokumen2 halamanChapter 196Dwi LestariBelum ada peringkat
- Follow UpDokumen5 halamanFollow UpDwi LestariBelum ada peringkat
- Chapter 196Dokumen2 halamanChapter 196Dwi LestariBelum ada peringkat
- Jurnal 7 Kelompok CDokumen18 halamanJurnal 7 Kelompok CDwi LestariBelum ada peringkat
- Lampiran Desain TurtleDokumen2 halamanLampiran Desain TurtleDwi LestariBelum ada peringkat
- Dentin - Pulp Complex Laboratory: Temple University School of MedicineDokumen12 halamanDentin - Pulp Complex Laboratory: Temple University School of MedicineDwi LestariBelum ada peringkat
- Dwi Lestari 04121401083Dokumen30 halamanDwi Lestari 04121401083Dwi LestariBelum ada peringkat
- Skenario G Blok 23 Tahun 2014Dokumen6 halamanSkenario G Blok 23 Tahun 2014Mandeep DhillonBelum ada peringkat
- Skenario G Blok 23 Tahun 2014Dokumen6 halamanSkenario G Blok 23 Tahun 2014Mandeep DhillonBelum ada peringkat
- Skenario C Blok 23Dokumen4 halamanSkenario C Blok 23Celcius ButandyBelum ada peringkat
- PRN Effectiveness PresentationDokumen14 halamanPRN Effectiveness Presentationapi-457177638Belum ada peringkat
- Breast Feeding ModifiedDokumen16 halamanBreast Feeding ModifiedTilahun Mikias100% (1)
- Sensitivity and SpecificityDokumen12 halamanSensitivity and Specificitymia farrowBelum ada peringkat
- Patient Delivery Receipt: Product Delivery Location: FacilityDokumen1 halamanPatient Delivery Receipt: Product Delivery Location: FacilityPat Dela CruzBelum ada peringkat
- Pudendal Neuralgia and Osteopathy Template1Dokumen3 halamanPudendal Neuralgia and Osteopathy Template1LauraBelum ada peringkat
- Aparat Elect Rot Era Pie Aries MDokumen2 halamanAparat Elect Rot Era Pie Aries MSorin NechiforBelum ada peringkat
- tmpD824 TMPDokumen12 halamantmpD824 TMPFrontiersBelum ada peringkat
- Marijuana and EpilepsyDokumen17 halamanMarijuana and EpilepsyOmar AntabliBelum ada peringkat
- CT and MRI of Abdomen and PelvicDokumen1.691 halamanCT and MRI of Abdomen and PelvicĐức Khang NguyễnBelum ada peringkat
- COPD Vs RLDDokumen64 halamanCOPD Vs RLDXine DeeBelum ada peringkat
- 5,600 Residents Tested: Case SummaryDokumen3 halaman5,600 Residents Tested: Case SummaryPeterborough ExaminerBelum ada peringkat
- 93092-Technique of Stent-Retriever Thrombectomy.Dokumen7 halaman93092-Technique of Stent-Retriever Thrombectomy.dediBelum ada peringkat
- Saunders, Et Al (2017)Dokumen9 halamanSaunders, Et Al (2017)uki arrownaraBelum ada peringkat
- Terlipressin Is Superior To Noradrenaline PDFDokumen11 halamanTerlipressin Is Superior To Noradrenaline PDFfcodoc321Belum ada peringkat
- CV Dr. Eko Arianto SpU 2021Dokumen10 halamanCV Dr. Eko Arianto SpU 2021Bedah ManadoBelum ada peringkat
- Brochure Biology & Medicine 03 2022 - CompressedDokumen40 halamanBrochure Biology & Medicine 03 2022 - CompressedMerida Bertrand Alex PodgaBelum ada peringkat
- Lesson Plan Genito UrinaryDokumen26 halamanLesson Plan Genito UrinaryEllen AngelBelum ada peringkat
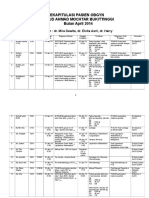
- Rekapitulasi Pasien Obgyn Apr 2014 2Dokumen20 halamanRekapitulasi Pasien Obgyn Apr 2014 2Ressy Dara AmeliaBelum ada peringkat
- Devoir de Synthèse N°2 2011 2012 (Lycée Ali Bourguiba Bembla)Dokumen4 halamanDevoir de Synthèse N°2 2011 2012 (Lycée Ali Bourguiba Bembla)ferchichi halimaBelum ada peringkat
- Health and Family Welfare (C) Department: PreambleDokumen14 halamanHealth and Family Welfare (C) Department: PreambleAjish BenjaminBelum ada peringkat
- Sensus Harian TGL 02 Maret 2022...........Dokumen121 halamanSensus Harian TGL 02 Maret 2022...........Ruhut Putra SinuratBelum ada peringkat
- Pre Op NCPDokumen1 halamanPre Op NCPJoshua Kelly0% (2)
- Twin Block 3Dokumen2 halamanTwin Block 3GisselaMaldonadoBelum ada peringkat
- Arihant Hospital & Research CentreDokumen30 halamanArihant Hospital & Research CentreSourabhSharmaBelum ada peringkat