Anda mungkin juga menyukai
- ARK - Meridian Focused TherapyDokumen29 halamanARK - Meridian Focused TherapySébastien Van100% (1)
- Mastering AutismDokumen320 halamanMastering AutismIulia Balutoiu100% (2)
- Unit1pptnotes 210823071031Dokumen65 halamanUnit1pptnotes 210823071031SAMPATH ABelum ada peringkat
- Ayaw Sigig Cellphone Oy! Priorities First! PRAY Lang!Dokumen6 halamanAyaw Sigig Cellphone Oy! Priorities First! PRAY Lang!Kenneth Mae Padual GullanBelum ada peringkat
- QT1 Tutorial 1-4 Student VersionDokumen11 halamanQT1 Tutorial 1-4 Student VersionSammie PingBelum ada peringkat
- Lasers in Ophthalmology: Moderator: Dr. S. Kalpana Presenter: Dr. AnjaliDokumen89 halamanLasers in Ophthalmology: Moderator: Dr. S. Kalpana Presenter: Dr. AnjaliSammie PingBelum ada peringkat
- Laser: Recent Advances in OtorhinolaryngologyDokumen65 halamanLaser: Recent Advances in OtorhinolaryngologyAnkushJainBelum ada peringkat
- Laserinophthalmology 180821172741Dokumen82 halamanLaserinophthalmology 180821172741Apps OmBelum ada peringkat
- Unit V R2019Dokumen46 halamanUnit V R2019Gayathri RadhaBelum ada peringkat
- Laser Applications To Medicine and BiologyDokumen56 halamanLaser Applications To Medicine and BiologyPunit RaiBelum ada peringkat
- 1 Introduction To Radiology, Brief HX & X Ray ProductionDokumen40 halaman1 Introduction To Radiology, Brief HX & X Ray ProductionMeraol HusseinBelum ada peringkat
- Laser RetinaDokumen70 halamanLaser RetinaSatya Hutama100% (1)
- X-Ray (General Idea)Dokumen11 halamanX-Ray (General Idea)Zahirul Ahsan ZahirBelum ada peringkat
- 20 Bio Medical LasersDokumen77 halaman20 Bio Medical Laserskaushik4208Belum ada peringkat
- Moderator: Dr. S. Kalpana Presenter: Dr. AnjaliDokumen89 halamanModerator: Dr. S. Kalpana Presenter: Dr. Anjaliايه سلام خضير عباس تقنيات البصرياتBelum ada peringkat
- Chap.1. Brief HX & X-Ray ProductionDokumen42 halamanChap.1. Brief HX & X-Ray ProductiongetemeselewBelum ada peringkat
- Laser Radiation HazardsDokumen16 halamanLaser Radiation HazardsLarryKnappBelum ada peringkat
- 8.2. EMW-source, Frequency Range, UsesDokumen3 halaman8.2. EMW-source, Frequency Range, UsesRamananBelum ada peringkat
- Laser Application: IntroductionDokumen8 halamanLaser Application: IntroductionArjay CarolinoBelum ada peringkat
- Remote Sensing - X-Ray NotesDokumen21 halamanRemote Sensing - X-Ray NotesJk JeeksBelum ada peringkat
- CBM355 Medical Imaging Systems 2-MarksDokumen23 halamanCBM355 Medical Imaging Systems 2-Markssanthosh sekar100% (2)
- Lasers in OphthalmologyDokumen33 halamanLasers in OphthalmologyBushra SherwaniBelum ada peringkat
- Radiology in Orthodontics-Dr - Kavitha / Orthodontic Courses by Indian Dental AcademyDokumen85 halamanRadiology in Orthodontics-Dr - Kavitha / Orthodontic Courses by Indian Dental Academyindian dental academyBelum ada peringkat
- Ophthalmology Femtosecond LaserDokumen8 halamanOphthalmology Femtosecond LaserChandrika MaluftiBelum ada peringkat
- Lasers in OphthalmologyDokumen15 halamanLasers in OphthalmologyMaliha KhanBelum ada peringkat
- Lasers in Ophthalmology Part - 1Dokumen53 halamanLasers in Ophthalmology Part - 1bhartiBelum ada peringkat
- Surgical Lasers PDFDokumen89 halamanSurgical Lasers PDFSammie PingBelum ada peringkat
- Lasers in Urology DR BiokuDokumen33 halamanLasers in Urology DR BiokumbiokuBelum ada peringkat
- Laser in OphthalmologyDokumen5 halamanLaser in Ophthalmologydykesu1806Belum ada peringkat
- Instruments For Optical SpectrometryDokumen2 halamanInstruments For Optical SpectrometrySean CollinsBelum ada peringkat
- Infrared Radiation On Ocular Tissue PDFDokumen7 halamanInfrared Radiation On Ocular Tissue PDFLeo KolongBelum ada peringkat
- Physics - Electromagnetic WavesDokumen3 halamanPhysics - Electromagnetic WavesALLU SRISAIBelum ada peringkat
- Laser in EntDokumen16 halamanLaser in EntKumar NeelakandanBelum ada peringkat
- Examen Ambrosio 2 InglesDokumen12 halamanExamen Ambrosio 2 InglesLadhy Guadalupe Feliciano FuentesBelum ada peringkat
- Chapter 1 RT TrainingDokumen4 halamanChapter 1 RT Trainingtek_surinderBelum ada peringkat
- Xray FundamentalsDokumen27 halamanXray FundamentalsABISHKAR SARKARBelum ada peringkat
- 1.01 Background Fundamentals For Diagnostic RadiologyDokumen4 halaman1.01 Background Fundamentals For Diagnostic RadiologyJason MirasolBelum ada peringkat
- Radiology Lec.1Dokumen67 halamanRadiology Lec.1ahmedBelum ada peringkat
- Abdullah Hussien TestDokumen9 halamanAbdullah Hussien Testfaris daboolBelum ada peringkat
- ScienceDokumen4 halamanScienceseradillajoshgabrielBelum ada peringkat
- EM WavesDokumen3 halamanEM WavesVansh SinghaiBelum ada peringkat
- Laser Uses in Plastic SurgeryDokumen70 halamanLaser Uses in Plastic Surgerygg.ganapathyBelum ada peringkat
- Applications of Laser in The Biomedical FieldDokumen26 halamanApplications of Laser in The Biomedical FieldAnikaBelum ada peringkat
- Lect. 1 Optical FiberDokumen12 halamanLect. 1 Optical FiberengshimaaBelum ada peringkat
- Uvr 03Dokumen57 halamanUvr 03Shruti ShahBelum ada peringkat
- Ultravoilet RadiationsDokumen54 halamanUltravoilet RadiationsNajeeb Ullah Qadir via GTXBelum ada peringkat
- Studies Photosynthesis: OF Using A Pulsed Laser I. Temperature Cytochrome ChromatiumDokumen23 halamanStudies Photosynthesis: OF Using A Pulsed Laser I. Temperature Cytochrome Chromatiumjames.devault5166Belum ada peringkat
- Physics of Laser:: Aser in OphthalmologyDokumen5 halamanPhysics of Laser:: Aser in OphthalmologyMariam QaisBelum ada peringkat
- Effect of Laser Pulse Duration On Damage To Metal Mirrors For Laser IFEDokumen8 halamanEffect of Laser Pulse Duration On Damage To Metal Mirrors For Laser IFEKimberly PerezBelum ada peringkat
- Notes On Radn and RadioactivityDokumen7 halamanNotes On Radn and RadioactivityYael Opeña AlipBelum ada peringkat
- Hospital Management AppDokumen12 halamanHospital Management AppAnu VinodBelum ada peringkat
- Notes On K Laser Certification Modules 2 2016Dokumen7 halamanNotes On K Laser Certification Modules 2 2016deni_yauka5540Belum ada peringkat
- Light: Jump To Navigation Jump To SearchDokumen4 halamanLight: Jump To Navigation Jump To SearchRonaldBelum ada peringkat
- X RayDokumen37 halamanX RayPriyank Dwivedi100% (1)
- Mid2 Sowjanya MamDokumen220 halamanMid2 Sowjanya MamArijit Dutta 210075698Belum ada peringkat
- Laser Lecture 3Dokumen29 halamanLaser Lecture 3yo391174Belum ada peringkat
- Chapter 5 - SEM and TEM - Lecture 1Dokumen28 halamanChapter 5 - SEM and TEM - Lecture 1majedBelum ada peringkat
- Electromagnetic WavesDokumen12 halamanElectromagnetic WavesINSIDIOUSBelum ada peringkat
- Electro Magnetic Waves M@trix FoundationDokumen7 halamanElectro Magnetic Waves M@trix FoundationdjbabuBelum ada peringkat
- Flocks - Laser Coagulation of Ocular TissuesDokumen8 halamanFlocks - Laser Coagulation of Ocular TissuesGeorge E. BozinisBelum ada peringkat
- Physics1101 - Course MaterialDokumen332 halamanPhysics1101 - Course MaterialAhmad RazaBelum ada peringkat
- Microwave Ra e PDFDokumen28 halamanMicrowave Ra e PDFSammie PingBelum ada peringkat
- Experiment O01 Chemical Properties of Alkenes: Results Table (Reaction of Cyclohexenes)Dokumen1 halamanExperiment O01 Chemical Properties of Alkenes: Results Table (Reaction of Cyclohexenes)Sammie PingBelum ada peringkat
- Surgical Lasers PDFDokumen89 halamanSurgical Lasers PDFSammie PingBelum ada peringkat
- Important Provisions in The Malaysian ConstitutionDokumen50 halamanImportant Provisions in The Malaysian ConstitutionSammie Ping50% (2)
- Ethnic Composition of The Malaysian PopulationDokumen56 halamanEthnic Composition of The Malaysian PopulationSammie PingBelum ada peringkat
- c2 PDFDokumen40 halamanc2 PDFSammie PingBelum ada peringkat
- The Supremacy of The ConstitutionDokumen24 halamanThe Supremacy of The ConstitutionSammie PingBelum ada peringkat
- Parliamentary Democracy in MalaysiaDokumen63 halamanParliamentary Democracy in MalaysiaWicky Yap0% (1)
- Carbohydrates - Key NotesDokumen3 halamanCarbohydrates - Key NotesSammie PingBelum ada peringkat
- (A) Outline The Need For Energy in Living Organisms, As Illustrated by Anabolicreactions, Active Transport, Movement and The Maintenance of Body TemperatureDokumen9 halaman(A) Outline The Need For Energy in Living Organisms, As Illustrated by Anabolicreactions, Active Transport, Movement and The Maintenance of Body TemperatureSammie PingBelum ada peringkat
- The Struggle For IndependenceDokumen93 halamanThe Struggle For IndependenceSammie PingBelum ada peringkat
- The Early History of MalaysiaDokumen94 halamanThe Early History of MalaysiaSammie PingBelum ada peringkat
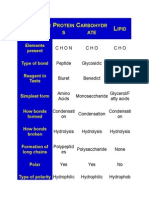
- C P C L: Haracteri Stic Rotein S Arbohydr ATE IpidDokumen2 halamanC P C L: Haracteri Stic Rotein S Arbohydr ATE IpidSammie PingBelum ada peringkat
- Medical English - Unit 18 VocabularyDokumen3 halamanMedical English - Unit 18 VocabularyAnna ClarkBelum ada peringkat
- Mddo PhysicianshandbookDokumen88 halamanMddo Physicianshandbookmary engBelum ada peringkat
- Final Defense PowerpointDokumen10 halamanFinal Defense PowerpointPaul CrucisBelum ada peringkat
- Art TherapyDokumen24 halamanArt Therapyfungperng100% (2)
- Treatment of Class II MalocclusionDokumen162 halamanTreatment of Class II Malocclusiongoyal8492% (13)
- NEEM As Mosquito ExpellantDokumen59 halamanNEEM As Mosquito Expellantknixau100% (2)
- Chapter 4Dokumen3 halamanChapter 4YZEL ALFECHEBelum ada peringkat
- Ssssihms PG Department Manual - Ortho DeptDokumen55 halamanSsssihms PG Department Manual - Ortho DeptshanmukhaBelum ada peringkat
- Building Regulations 2000 Part HDokumen62 halamanBuilding Regulations 2000 Part HEdwinHanBelum ada peringkat
- Sodium Lignosulfonate MSDS: Section 1: Chemical Product and Company IdentificationDokumen5 halamanSodium Lignosulfonate MSDS: Section 1: Chemical Product and Company IdentificationYasdiOKBelum ada peringkat
- Building Self-Compassion - 03 - Preparing For Self-CompassionDokumen9 halamanBuilding Self-Compassion - 03 - Preparing For Self-CompassionThe Happy Mind HouseBelum ada peringkat
- Hygiene 2Dokumen41 halamanHygiene 2Nermine ElcokanyBelum ada peringkat
- Stroke System of Care FinalDokumen3 halamanStroke System of Care FinalRamanathan KirthivasanBelum ada peringkat
- Role of Herbs in Endodontics: An Update: Endodontology Endodontology Endodontology Endodontology EndodontologyDokumen5 halamanRole of Herbs in Endodontics: An Update: Endodontology Endodontology Endodontology Endodontology EndodontologyDébora LimaBelum ada peringkat
- Prognosis and Discharge Plan - MaiaDokumen12 halamanPrognosis and Discharge Plan - Maiajia88100% (1)
- Gary Null Robert Houston Penthouse Magazine 1979 - Great Cancer FraudDokumen9 halamanGary Null Robert Houston Penthouse Magazine 1979 - Great Cancer FraudAnonymous AWVQB8ccJBelum ada peringkat
- Principles Cancer Systemic TherapyDokumen57 halamanPrinciples Cancer Systemic TherapyKarimina50% (2)
- DR - Nuha Alshammari Consultant Psychiatrist: First Episode Psychosis/Youth Crisis ManagementDokumen46 halamanDR - Nuha Alshammari Consultant Psychiatrist: First Episode Psychosis/Youth Crisis ManagementaliBelum ada peringkat
- Welcome To The Seminar ON: By: MARIA ABRAHAM (19093252)Dokumen22 halamanWelcome To The Seminar ON: By: MARIA ABRAHAM (19093252)Elna AbrahamBelum ada peringkat
- Common Ocular EmergenciesDokumen33 halamanCommon Ocular EmergenciesMaimoona AimanBelum ada peringkat
- Emotional Freedom Technique (EFT) - Emotional HealthDokumen47 halamanEmotional Freedom Technique (EFT) - Emotional Healthjose100% (3)
- Aapm TG 25Dokumen40 halamanAapm TG 25AnjihartsBelum ada peringkat
- 136 Management of Major Haemorrhage Part 1Dokumen6 halaman136 Management of Major Haemorrhage Part 1fitrah fajrianiBelum ada peringkat
- Cardex Diet:: Date/Time Treatment IVF Labs ProceduresDokumen1 halamanCardex Diet:: Date/Time Treatment IVF Labs ProceduresWeng RamojalBelum ada peringkat
- Course No.: BIOF216 Course Title: Water, Sanitation and Solid Waste ManagementDokumen6 halamanCourse No.: BIOF216 Course Title: Water, Sanitation and Solid Waste ManagementJeswin EldhoBelum ada peringkat
- PWC Managing Innovation Pharma PDFDokumen20 halamanPWC Managing Innovation Pharma PDFAryan RsBelum ada peringkat
- Listening Sample Test 3 Question PaperDokumen5 halamanListening Sample Test 3 Question PaperjeznerBelum ada peringkat
- Uroradiology Tutorial For Medical Students: Lesson 1: Ultrasound - Part 1 American Urological AssociationDokumen68 halamanUroradiology Tutorial For Medical Students: Lesson 1: Ultrasound - Part 1 American Urological AssociationDavid CiempkaBelum ada peringkat