Anda mungkin juga menyukai
- Floating ElbowDokumen5 halamanFloating ElbowpepitomuraBelum ada peringkat
- Avascular Necrosis and Related Complications Following Healed Osteoporotic Intertrochanteric FracturesDokumen4 halamanAvascular Necrosis and Related Complications Following Healed Osteoporotic Intertrochanteric FracturesNasrull BinHzBelum ada peringkat
- Ijcmsr 312 v1Dokumen7 halamanIjcmsr 312 v1AshliiqueBelum ada peringkat
- Conservative Treatment of Medial Shaft Clavicle Fracture With Borderline Criteria A Case ReportDokumen9 halamanConservative Treatment of Medial Shaft Clavicle Fracture With Borderline Criteria A Case ReportAthenaeum Scientific PublishersBelum ada peringkat
- 35 Daksh EtalDokumen4 halaman35 Daksh EtaleditorijmrhsBelum ada peringkat
- Ankle Syndesmotic InjuryDokumen10 halamanAnkle Syndesmotic InjuryC Martin TraumatoBelum ada peringkat
- Knee Injury Evaluation Radiology PerspectiveDokumen14 halamanKnee Injury Evaluation Radiology PerspectiveOctavian CatanăBelum ada peringkat
- Clavicle FractureDokumen6 halamanClavicle FractureYbis LizarzaburuBelum ada peringkat
- Anterior Cruciate Ligament Rupture and Osteoarthritis ProgressionDokumen6 halamanAnterior Cruciate Ligament Rupture and Osteoarthritis ProgressionHendry BarcaBelum ada peringkat
- Fraktur Klavikula PDFDokumen15 halamanFraktur Klavikula PDFSJ Iraa100% (1)
- 10n9n9dDokumen9 halaman10n9n9dAde Triansyah EmsilBelum ada peringkat
- Management of The Mangled ExtremityDokumen10 halamanManagement of The Mangled ExtremityosteonectinBelum ada peringkat
- Tools For Diagnosis of Knee InjuriesDokumen10 halamanTools For Diagnosis of Knee Injuriesmanjukumard2007Belum ada peringkat
- Art3a10 10072fs00256-014-1842-5Dokumen9 halamanArt3a10 10072fs00256-014-1842-5api-253958760Belum ada peringkat
- Fraktur AnkleDokumen60 halamanFraktur AnkleAries RHBelum ada peringkat
- Acta Orthopaedica Et Traumatologica TurcicaDokumen6 halamanActa Orthopaedica Et Traumatologica TurcicaAnonymous TvPFA4Belum ada peringkat
- Primary Traumatic Patellar DislocationDokumen6 halamanPrimary Traumatic Patellar DislocationOgirahma T. NaidBelum ada peringkat
- The Stiff Elbow PDFDokumen17 halamanThe Stiff Elbow PDFanindhita anestyaBelum ada peringkat
- Lumbar Spine Trauma Imaging - Overview, Radiography, Computed TomographyDokumen36 halamanLumbar Spine Trauma Imaging - Overview, Radiography, Computed TomographyAchmadRizaBelum ada peringkat
- Evaluation of Elbow Pain in AdultsDokumen9 halamanEvaluation of Elbow Pain in AdultsJuan Sebastián Montaño MaldonadoBelum ada peringkat
- Morbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesDokumen8 halamanMorbidity and Total Knee Arthroplasty As A Long Term Sequela of Tibial Plateau FracturesAthenaeum Scientific PublishersBelum ada peringkat
- Surgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009Dokumen6 halamanSurgical Outcomes After Traumatic Open Knee Dislocation: Ó Springer-Verlag 2009agus sukarnaBelum ada peringkat
- Credibility of Three Column Fixation in Schatzker Types V and VI Tibial Plateau FracturesDokumen6 halamanCredibility of Three Column Fixation in Schatzker Types V and VI Tibial Plateau FracturesInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Com Minuted Patellar FractureDokumen3 halamanCom Minuted Patellar FractureAhmet EkinciBelum ada peringkat
- Our Experience in Meniscus Tears and Differences in Sport Recovery Between Medial and Lateral Partial Meniscectomy in Young AthleteDokumen11 halamanOur Experience in Meniscus Tears and Differences in Sport Recovery Between Medial and Lateral Partial Meniscectomy in Young AthleteAthenaeum Scientific PublishersBelum ada peringkat
- Ortiz 2016Dokumen23 halamanOrtiz 2016Tomás Urrutia JarpaBelum ada peringkat
- Evaluation and Treatment of Ankle SprainsDokumen11 halamanEvaluation and Treatment of Ankle SprainsMariana MonauniBelum ada peringkat
- Carpometacarpal Dislocation of The Thumb Associated With Fracture of The TrapeziumDokumen5 halamanCarpometacarpal Dislocation of The Thumb Associated With Fracture of The TrapeziumPuputBelum ada peringkat
- 6 - Injuries To The Ulnar Collateral Ligament o - 2018 - Clinical Orthopaedic Re PDFDokumen4 halaman6 - Injuries To The Ulnar Collateral Ligament o - 2018 - Clinical Orthopaedic Re PDFTolo CantallopsBelum ada peringkat
- Research ArticleDokumen5 halamanResearch ArticleZirco HereBelum ada peringkat
- Thesis Umesh A2z.doc Final Thesis CorrectionDokumen79 halamanThesis Umesh A2z.doc Final Thesis CorrectionRakesh JhaBelum ada peringkat
- Acl Recon With BPT GraftDokumen6 halamanAcl Recon With BPT Graftpaper coe medanBelum ada peringkat
- MDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewDokumen9 halamanMDCT and MRI Evaluation of Cervical Spine Trauma: Pictorial ReviewcalinmariusBelum ada peringkat
- The Terrible Triad of The ElbowDokumen5 halamanThe Terrible Triad of The Elbowapi-250084607Belum ada peringkat
- Plantillo Anteromedial + LCP + ApeDokumen7 halamanPlantillo Anteromedial + LCP + ApeThiagoBelum ada peringkat
- Cartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesDari EverandCartilage Injury of the Knee: State-of-the-Art Treatment and ControversiesAaron J. KrychBelum ada peringkat
- The Meniscus in Kne e Osteoarthritis: Martin Englund,, Ali Guermazi,, L. Stefan LohmanderDokumen12 halamanThe Meniscus in Kne e Osteoarthritis: Martin Englund,, Ali Guermazi,, L. Stefan LohmanderNati GallardoBelum ada peringkat
- Case Report: A Rare Case of Bilateral Patellar Tendon Ruptures: A Case Report and Literature ReviewDokumen4 halamanCase Report: A Rare Case of Bilateral Patellar Tendon Ruptures: A Case Report and Literature ReviewOBLIVION_29Belum ada peringkat
- Falling From The Tightrope: Double Versus Single Tightropes in Patients With Acromioclavicular Joint Dislocations: Technique and ComplicationsDokumen6 halamanFalling From The Tightrope: Double Versus Single Tightropes in Patients With Acromioclavicular Joint Dislocations: Technique and ComplicationsChrysi TsiouriBelum ada peringkat
- Tibial Spine Avulsion Fractures: Current Concepts and Technical Note On Arthroscopic Techniques Used in Management of These InjuriesDokumen16 halamanTibial Spine Avulsion Fractures: Current Concepts and Technical Note On Arthroscopic Techniques Used in Management of These InjuriesGeraldine Alvarez ABelum ada peringkat
- Fifteen-Year To 19-Year Follow-Up of The Insall-Burstein-1 Total Knee ArthroplastyDokumen6 halamanFifteen-Year To 19-Year Follow-Up of The Insall-Burstein-1 Total Knee ArthroplastyFajar BascBelum ada peringkat
- Ankle SprainsDokumen18 halamanAnkle Sprainsnelson1313Belum ada peringkat
- Articular Fractures of The Distal HumerusDokumen9 halamanArticular Fractures of The Distal HumerusJoha DavilaBelum ada peringkat
- The Relationship Between Anterior Cruciate Ligament Injury and Osteoarthritis of The KneeDokumen12 halamanThe Relationship Between Anterior Cruciate Ligament Injury and Osteoarthritis of The KneeMufidAljaruBelum ada peringkat
- A Galeazzi-Variant Type Fracture-Dislocation in Adults: Results: All Cases Were Followed Up For 24 Weeks. TheDokumen3 halamanA Galeazzi-Variant Type Fracture-Dislocation in Adults: Results: All Cases Were Followed Up For 24 Weeks. TheTruly GracevaBelum ada peringkat
- 10.1177 1941738110397875 PDFDokumen16 halaman10.1177 1941738110397875 PDFalwy sugiartoBelum ada peringkat
- Ankle Fractures: A Literature Review of Current Treatment MethodsDokumen13 halamanAnkle Fractures: A Literature Review of Current Treatment Methodsadrian1989Belum ada peringkat
- International Journal of Advances in Case ReportsDokumen3 halamanInternational Journal of Advances in Case ReportsastritriBelum ada peringkat
- Anterior Cruciate Ligament ImagingDokumen10 halamanAnterior Cruciate Ligament Imagingjohari23Belum ada peringkat
- Z Effect & Reverse Z Effect in PFNDokumen7 halamanZ Effect & Reverse Z Effect in PFNNandan SurBelum ada peringkat
- Clasificaciòn Esguince de TobilloDokumen11 halamanClasificaciòn Esguince de TobilloWilliams BalboaBelum ada peringkat
- DL TPSFDokumen5 halamanDL TPSFPramod N KBelum ada peringkat
- Bilateral Radial Neck Fracture - Rare Case ReportDokumen2 halamanBilateral Radial Neck Fracture - Rare Case ReportIOSRjournalBelum ada peringkat
- 37886153Dokumen22 halaman37886153Zilbran BerontaxBelum ada peringkat
- Case Series OIDokumen6 halamanCase Series OIJulius JuliusBelum ada peringkat
- 2020 Finite Element Analysis - Femur Malunion+knee OADokumen9 halaman2020 Finite Element Analysis - Femur Malunion+knee OAstudmmaBelum ada peringkat
- Anderson and Anderson, 2011Dokumen16 halamanAnderson and Anderson, 2011Salsabila Kusuma JannatiBelum ada peringkat
- Pfirrmann VariantsPitfallsWristImaging EJR 56 2005Dokumen10 halamanPfirrmann VariantsPitfallsWristImaging EJR 56 2005Pankaj NarekarBelum ada peringkat
- InTech-Knee Pain in Adults Adolescents Diagnosis and TreatmentDokumen32 halamanInTech-Knee Pain in Adults Adolescents Diagnosis and Treatmentevil freakBelum ada peringkat
- j1q82016Dokumen4 halamanj1q82016ichkhuyBelum ada peringkat
- j1q82016Dokumen4 halamanj1q82016ichkhuyBelum ada peringkat
- M.O.E.M.S Practice Packet 1998-1999Dokumen11 halamanM.O.E.M.S Practice Packet 1998-1999ichkhuyBelum ada peringkat
- Foot and Ankle Questions On The OrthopaedicDokumen9 halamanFoot and Ankle Questions On The OrthopaedicichkhuyBelum ada peringkat
- South African Mathematics Olympiad Grade EIGHT First Round 2016 SolutionsDokumen2 halamanSouth African Mathematics Olympiad Grade EIGHT First Round 2016 SolutionsichkhuyBelum ada peringkat
- SAMO Junior 2015 To 1998 QuestionsDokumen301 halamanSAMO Junior 2015 To 1998 Questionsichkhuy69% (16)
- The South African Mathematics Olympiad Senior Second Round 2015 SolutionsDokumen5 halamanThe South African Mathematics Olympiad Senior Second Round 2015 SolutionsichkhuyBelum ada peringkat
- 11 - 16 - 2016 Scientific Overall Program of SCC VUTHY - Draft EnglishDokumen16 halaman11 - 16 - 2016 Scientific Overall Program of SCC VUTHY - Draft EnglishichkhuyBelum ada peringkat
- South African Mathematics FoundationDokumen7 halamanSouth African Mathematics FoundationichkhuyBelum ada peringkat
- MOCPVol2 SampleDokumen11 halamanMOCPVol2 SampleSadi Snmz67% (3)
- Mathematics Olympiad Set 2Dokumen21 halamanMathematics Olympiad Set 2ichkhuyBelum ada peringkat
- SASMO 2014 Round 1 Primary 2 SolutionsDokumen6 halamanSASMO 2014 Round 1 Primary 2 Solutionsichkhuy100% (7)
- Kvs Jmo 2009 6Dokumen1 halamanKvs Jmo 2009 6ichkhuyBelum ada peringkat
- Kvs Jmo 2009 5Dokumen3 halamanKvs Jmo 2009 5ichkhuyBelum ada peringkat
- APSMO Olympiad Sample DivS 1Dokumen2 halamanAPSMO Olympiad Sample DivS 1ichkhuyBelum ada peringkat
- APSMO Olympiad Sample DivJ 1Dokumen2 halamanAPSMO Olympiad Sample DivJ 1ichkhuy0% (1)
- APSMO Olympiad Sample DivJ 1Dokumen2 halamanAPSMO Olympiad Sample DivJ 1ichkhuy0% (1)
- Hong Kong Mathematical Olympiad Association: SASMO Sample Paper (S2) AnswerDokumen1 halamanHong Kong Mathematical Olympiad Association: SASMO Sample Paper (S2) AnswerichkhuyBelum ada peringkat
- SASMO 2014 Round 1 Primary 2 ProblemsDokumen2 halamanSASMO 2014 Round 1 Primary 2 Problemsichkhuy88% (8)
- Expt 2007 PDFDokumen26 halamanExpt 2007 PDFichkhuyBelum ada peringkat
- Resume For TransitionDokumen1 halamanResume For Transitionapi-659158323Belum ada peringkat
- Fernandez Doctor - Goya's Mental Illness 1994Dokumen6 halamanFernandez Doctor - Goya's Mental Illness 1994FranciscoBelum ada peringkat
- Medical-Surgical Nusing Checklist: Conams Wesleyan University Philippines 2020-2021Dokumen17 halamanMedical-Surgical Nusing Checklist: Conams Wesleyan University Philippines 2020-2021Sheena Allana AngelesBelum ada peringkat
- Quiz Comprehension and Error Identification W2Dokumen3 halamanQuiz Comprehension and Error Identification W2norlianaBelum ada peringkat
- Microteaching: MDR - TBDokumen16 halamanMicroteaching: MDR - TBVikram Singh RanawatBelum ada peringkat
- Introduction To Art Therapy Research (By Lynn Kapitan)Dokumen104 halamanIntroduction To Art Therapy Research (By Lynn Kapitan)td100% (1)
- September 05, 2022 - September 09, 2022Dokumen2 halamanSeptember 05, 2022 - September 09, 2022Maybelyn de los ReyesBelum ada peringkat
- Sample Correction Nursing 300Dokumen2 halamanSample Correction Nursing 300Dandlers MurrayBelum ada peringkat
- Puneti Verbele Din Urmatoarele Propozitii (PRESENT CONTINUOUS) La Negativ Si InterogativDokumen2 halamanPuneti Verbele Din Urmatoarele Propozitii (PRESENT CONTINUOUS) La Negativ Si Interogativflori grosuBelum ada peringkat
- Physicians Directory PDFDokumen126 halamanPhysicians Directory PDFThebestearldom0% (1)
- Test Bank For Cultural Diversity in Health and Illness 8th Edition Rachel e SpectorDokumen25 halamanTest Bank For Cultural Diversity in Health and Illness 8th Edition Rachel e SpectorCatherine Smith100% (33)
- Nursing Care Plan AppendicitisDokumen2 halamanNursing Care Plan Appendicitisderic95% (57)
- Standard 13Dokumen22 halamanStandard 13Bridget Gumbo100% (1)
- 特 定 技 能 外 国 人 の 履 歴 書 Curriculum Vitae Of The Specified Skilled WorkerDokumen25 halaman特 定 技 能 外 国 人 の 履 歴 書 Curriculum Vitae Of The Specified Skilled WorkerAoi BaraBelum ada peringkat
- Pas Big Ganjil 2022 Kls 9 Edit BIMA 40 Nomer + 5 ESSAYDokumen7 halamanPas Big Ganjil 2022 Kls 9 Edit BIMA 40 Nomer + 5 ESSAYSyamsul ArifinBelum ada peringkat
- Basic Concepts of Nutrition and Diet TherapyDokumen4 halamanBasic Concepts of Nutrition and Diet TherapybananakyuBelum ada peringkat
- Sense Memory 11: Private MomentDokumen5 halamanSense Memory 11: Private MomentJonathan Samarro100% (4)
- The Cecil Kelley Criticality AccidentDokumen2 halamanThe Cecil Kelley Criticality AccidentAnand AbrahamBelum ada peringkat
- Human Resource MGMT 556 v1Dokumen330 halamanHuman Resource MGMT 556 v1jugal bariBelum ada peringkat
- NCM 100 SKILLS Nursing Process HandoutsDokumen10 halamanNCM 100 SKILLS Nursing Process HandoutsPearl IbisateBelum ada peringkat
- Usia Dan ParitasDokumen16 halamanUsia Dan ParitasNurulismi SubbeBelum ada peringkat
- P4 ScienceDokumen48 halamanP4 ScienceRonald SsuunaBelum ada peringkat
- WHO MSD GSEDpackage v1.0 2023.1 Eng PDFDokumen60 halamanWHO MSD GSEDpackage v1.0 2023.1 Eng PDFGoteti NaliniBelum ada peringkat
- FLORIDA DEPARTMENT OF CHILDREN AND FAMILIES Statement of Estimated Regulatory Costs (SERC)Dokumen12 halamanFLORIDA DEPARTMENT OF CHILDREN AND FAMILIES Statement of Estimated Regulatory Costs (SERC)The Federalist100% (1)
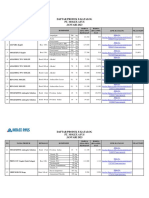
- Daftar Harga E-Katalog - Pt. Molex Ayus - Januari 2023-1Dokumen2 halamanDaftar Harga E-Katalog - Pt. Molex Ayus - Januari 2023-1AmmilaMasruriRahmawatiBelum ada peringkat
- Neurologic DisordersDokumen3 halamanNeurologic Disordersjojimar08Belum ada peringkat
- Puti Mustika Swandyani, Agus Santoso, Yohanes KristiantoDokumen11 halamanPuti Mustika Swandyani, Agus Santoso, Yohanes KristiantoAnonimBelum ada peringkat
- Pros and Cons of Research in E.H.Dokumen3 halamanPros and Cons of Research in E.H.goldMINDBelum ada peringkat
- NURS FPX 6030 Assessment 5 Evaluation Plan DesignDokumen4 halamanNURS FPX 6030 Assessment 5 Evaluation Plan DesignEmma WatsonBelum ada peringkat
- Components of Food-Questions and AnswersDokumen3 halamanComponents of Food-Questions and Answersmahesh_mymailBelum ada peringkat