Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Nasm Study Guide PDF 2016 Nasm CPTDokumen54 halamanNasm Study Guide PDF 2016 Nasm CPTSarvpreet SinghBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Comprehensive Classification of Fragility Fractures of The Pelvic Ring: Recommendations For Surgical TreatmentDokumen12 halamanComprehensive Classification of Fragility Fractures of The Pelvic Ring: Recommendations For Surgical TreatmentEmanuele CiurliaBelum ada peringkat
- James Ray Dixon - Amphibians and Reptiles of Texas - With Keys, Taxonomic Synopses, Bibliography, and Distribution Maps (W.L. Moody, JR., Natural History Series, No. 8.) (2000) PDFDokumen430 halamanJames Ray Dixon - Amphibians and Reptiles of Texas - With Keys, Taxonomic Synopses, Bibliography, and Distribution Maps (W.L. Moody, JR., Natural History Series, No. 8.) (2000) PDFjohannesBelum ada peringkat
- 43 Extra Acupuncture PointsDokumen3 halaman43 Extra Acupuncture PointsIndra Syafri100% (3)
- Real-Life Assessment of The Multidimensional Nature of Dyspnoea in COPD OutpatientsDokumen12 halamanReal-Life Assessment of The Multidimensional Nature of Dyspnoea in COPD OutpatientsRaúl Ferrer PeñaBelum ada peringkat
- Receiver Operating Characteristic (ROC) Curve For Medical ResearchersDokumen11 halamanReceiver Operating Characteristic (ROC) Curve For Medical ResearchersRaúl Ferrer PeñaBelum ada peringkat
- Developmental Articles Primary Health Care and Community Based Rehabilitation: Implications For Physical TherapyDokumen33 halamanDevelopmental Articles Primary Health Care and Community Based Rehabilitation: Implications For Physical TherapyRaúl Ferrer PeñaBelum ada peringkat
- Reliability of Physical Examination For Diagnosis of Myofascial Trigger Points - A Systematic Review of The LiteratureDokumen10 halamanReliability of Physical Examination For Diagnosis of Myofascial Trigger Points - A Systematic Review of The LiteratureRaúl Ferrer PeñaBelum ada peringkat
- The Direction of Optimal Skin IncisionsDokumen11 halamanThe Direction of Optimal Skin Incisionsdrgurpal74Belum ada peringkat
- Bunn (2007) Meat Made Us Human PDFDokumen11 halamanBunn (2007) Meat Made Us Human PDFSam OstroffBelum ada peringkat
- Heath Carter ManualDokumen26 halamanHeath Carter ManualKyp KermanyBelum ada peringkat
- Equine Dissertation ExamplesDokumen6 halamanEquine Dissertation ExamplesWriteMyEnglishPaperChicago100% (1)
- CirugiaDokumen27 halamanCirugiaalexmtzgBelum ada peringkat
- Introduction To HAP: by Dr. Mrs. Deepa K. Ingawale (Mandlik) Department of Pharmacology Poona College of Pharmacy, PuneDokumen47 halamanIntroduction To HAP: by Dr. Mrs. Deepa K. Ingawale (Mandlik) Department of Pharmacology Poona College of Pharmacy, PunePrathi100% (2)
- Colon in Loop English VersionDokumen16 halamanColon in Loop English Versionnyla trBelum ada peringkat
- Removable Denture Prosthetics - Technical Protocol PDFDokumen42 halamanRemovable Denture Prosthetics - Technical Protocol PDFDaniel DidiBelum ada peringkat
- Brownies RecipeDokumen2 halamanBrownies RecipeMrTakbaBelum ada peringkat
- Intro To Ortho Anatomy PDFDokumen55 halamanIntro To Ortho Anatomy PDFlanghalilafaBelum ada peringkat
- A Review of Normal Radiographical Variants Commonly Mistaken For Pathological Findings in HorsesDokumen9 halamanA Review of Normal Radiographical Variants Commonly Mistaken For Pathological Findings in HorsesI KBelum ada peringkat
- Alan Pipe: Archaeological Animal Bone On The Thames Foreshore - Techniques and LimitationsDokumen36 halamanAlan Pipe: Archaeological Animal Bone On The Thames Foreshore - Techniques and LimitationsThames Discovery ProgrammeBelum ada peringkat
- CH 01 Lecture PresentationDokumen90 halamanCH 01 Lecture PresentationNie TofuBelum ada peringkat
- Frotis SanguineoDokumen4 halamanFrotis SanguineoMarcos RosalesBelum ada peringkat
- F1223 1479757-1Dokumen9 halamanF1223 1479757-1Thaweekarn ChangthongBelum ada peringkat
- Anatomy: ST ND TH TH Th. RD TH TH THDokumen11 halamanAnatomy: ST ND TH TH Th. RD TH TH THskBelum ada peringkat
- 16 Complex Odontogenic Infections PDFDokumen13 halaman16 Complex Odontogenic Infections PDFDori SanchezBelum ada peringkat
- Validation The Long Sitting Test On Subjects With Lliosacral DysfunctionDokumen10 halamanValidation The Long Sitting Test On Subjects With Lliosacral Dysfunction黃郁庭Belum ada peringkat
- Chest RadiographyDokumen19 halamanChest RadiographyClaraMonet PalomoBelum ada peringkat
- 1 Week - Laboratory ExercisesDokumen83 halaman1 Week - Laboratory ExercisesGeevee Naganag VentulaBelum ada peringkat
- Human Physiology: Level of Structural Organization of The BodyDokumen6 halamanHuman Physiology: Level of Structural Organization of The Bodyhasan satchetBelum ada peringkat
- Pe 2 Course Pack - ExerciseDokumen50 halamanPe 2 Course Pack - ExerciseLOUISE DOROTHY PARAISOBelum ada peringkat
- PATH505PDokumen11 halamanPATH505PMohsin SialBelum ada peringkat
- Gosner TabelaDokumen9 halamanGosner TabelaEdicarlos Pralon SilvaBelum ada peringkat
- Pathological ReflexesDokumen2 halamanPathological ReflexesNilo Carmelo LumanogBelum ada peringkat
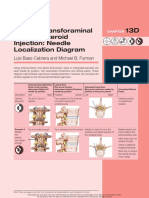
- Lumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramDokumen2 halamanLumbar Transforaminal Epidural Steroid Injection: Needle Localization DiagramSoumabho DasBelum ada peringkat