Anda mungkin juga menyukai
- Conn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandConn Syndrome, (Hyper-Aldosteronism) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- (PHYSIO B) 1.2 Renal Physio Pt. 3Dokumen8 halaman(PHYSIO B) 1.2 Renal Physio Pt. 3miguel cuevasBelum ada peringkat
- Renal Physiology: Done byDokumen28 halamanRenal Physiology: Done byJanine Marie Kathleen Uy-CuanangBelum ada peringkat
- Tubular Functions of KidneyDokumen161 halamanTubular Functions of KidneyPhysiology by Dr RaghuveerBelum ada peringkat
- Haemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)Dokumen20 halamanHaemotology Notes Haemotology Notes: Medicine (University of Glasgow) Medicine (University of Glasgow)shravaniBelum ada peringkat
- Gallbladder and Pancrease PathologyDokumen4 halamanGallbladder and Pancrease Pathologyjohn smithBelum ada peringkat
- (Pedia 3A) NEPHRO COMPILED PDFDokumen40 halaman(Pedia 3A) NEPHRO COMPILED PDFNoreenBelum ada peringkat
- Haematology - Blood Films.Dokumen6 halamanHaematology - Blood Films.kkkssbbBelum ada peringkat
- ARF HandoutDokumen29 halamanARF HandoutJoel Topf100% (6)
- Physio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionDokumen5 halamanPhysio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionAnny AlvrzBelum ada peringkat
- Medical School Renal ReviewDokumen32 halamanMedical School Renal ReviewwmtxbbBelum ada peringkat
- DR Najeeb Cardiac CycleDokumen5 halamanDR Najeeb Cardiac Cycleعلي. احمد100% (1)
- Chapter 13 Neoplastic Proliferations of White CellsDokumen16 halamanChapter 13 Neoplastic Proliferations of White CellsOmar100% (1)
- Haematology-Summary My NotesDokumen24 halamanHaematology-Summary My NotesToria053Belum ada peringkat
- Renal PhysiologyDokumen129 halamanRenal PhysiologynehaBelum ada peringkat
- Blood Components Where Do They Come From?: Introduction To HaematologyDokumen11 halamanBlood Components Where Do They Come From?: Introduction To Haematologydorsa koraeiBelum ada peringkat
- Renal PathologyDokumen5 halamanRenal PathologyEmmanuel De LeonBelum ada peringkat
- Renal PathologyDokumen28 halamanRenal PathologyApril Deveras JudillaBelum ada peringkat
- A&P 302 - Respiratory NotesDokumen31 halamanA&P 302 - Respiratory NotesBethanyBelum ada peringkat
- 18 Vessels and Flow DynamicsDokumen57 halaman18 Vessels and Flow Dynamicsraanja2Belum ada peringkat
- Basic Examination of Urine - Dr. PinedaDokumen20 halamanBasic Examination of Urine - Dr. PinedaElei GarciaBelum ada peringkat
- CHAPTER 35 AntigensAgglutinogensDokumen2 halamanCHAPTER 35 AntigensAgglutinogensg_komolafe100% (1)
- Q. List Different Functions of The Kidney: (A) Homeostatic FunctionDokumen42 halamanQ. List Different Functions of The Kidney: (A) Homeostatic Functionramadan100% (4)
- 2 - Renal PhysiologyDokumen8 halaman2 - Renal PhysiologyKunware TropaBelum ada peringkat
- 1 Patho5 - Kidney I 2015bDokumen10 halaman1 Patho5 - Kidney I 2015bmiguel cuevasBelum ada peringkat
- UrinalysisDokumen9 halamanUrinalysisSukma EffendyBelum ada peringkat
- Respiratory Physio UsmleDokumen61 halamanRespiratory Physio UsmleDr.G.Bhanu Prakash100% (2)
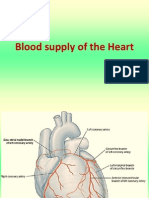
- Blood Supply of HeartDokumen7 halamanBlood Supply of Heartmariposa_0612Belum ada peringkat
- Glomerular Filtration Rate Factors and Regulation in 40 CharactersDokumen3 halamanGlomerular Filtration Rate Factors and Regulation in 40 CharactersPriscilia FooBelum ada peringkat
- FBC Interpretation and Function of Blood ComponentsDokumen7 halamanFBC Interpretation and Function of Blood ComponentsFrancesca LiBelum ada peringkat
- Plasma Physiology (1-2020) by DR Khaled A AbulfadleDokumen9 halamanPlasma Physiology (1-2020) by DR Khaled A AbulfadleUzama Binu AliBelum ada peringkat
- Physio Coursepack 2016Dokumen282 halamanPhysio Coursepack 2016Amanda KimBelum ada peringkat
- Lecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiDokumen41 halamanLecture On Blood Groups, Transfusion, RH Incompatibility by Dr. RoomiMudassar Roomi100% (1)
- Complete Urinalysis and Urine Test-2Dokumen34 halamanComplete Urinalysis and Urine Test-2azuraBelum ada peringkat
- Parathyroid Disease Lecture SlidesDokumen50 halamanParathyroid Disease Lecture SlidesMaxwell PalSingh100% (1)
- MHC I Proteins, Which Present Antigens To Cytotoxic T Cells, (2) MHC II Proteins, Which Present Antigens T Helper CellsDokumen25 halamanMHC I Proteins, Which Present Antigens To Cytotoxic T Cells, (2) MHC II Proteins, Which Present Antigens T Helper CellsMudassar Roomi100% (1)
- CNS Physiology LectureDokumen25 halamanCNS Physiology Lectureجبار هاوش عضيرس100% (1)
- Adrenal Cortex DR - GomezDokumen13 halamanAdrenal Cortex DR - Gomezvicbart11Belum ada peringkat
- The Complement SystemDokumen24 halamanThe Complement Systemhkatniwala100% (1)
- IV Fluid ChartDokumen2 halamanIV Fluid Chartbenny christantoBelum ada peringkat
- Disseminated Intravascular Coagulation (DIC) : Alyssa CardinalDokumen15 halamanDisseminated Intravascular Coagulation (DIC) : Alyssa CardinalAlyssa Cardinal100% (1)
- Robbins Ch. 18 Liver and Biliary Tract Review QuestionsDokumen12 halamanRobbins Ch. 18 Liver and Biliary Tract Review QuestionsPA2014Belum ada peringkat
- Glomerular FiltrationDokumen3 halamanGlomerular FiltrationyolandadwiooBelum ada peringkat
- Xray AbdominalDokumen38 halamanXray Abdominalrizki sanBelum ada peringkat
- Digestive System IDokumen15 halamanDigestive System IElena Arvaniti100% (1)
- Endocrinology NotesDokumen12 halamanEndocrinology Notesrandiey john abelleraBelum ada peringkat
- Acid-Base Balance ExplainedDokumen8 halamanAcid-Base Balance ExplainedNicole TangcoBelum ada peringkat
- Apoptosis by Dr. Sanjiv Kumar-1Dokumen27 halamanApoptosis by Dr. Sanjiv Kumar-1चौधरी हरिओम सौरोतBelum ada peringkat
- Pediatric Renal TraumaDokumen26 halamanPediatric Renal Traumatepat rshsBelum ada peringkat
- 3rd Lecture On Nerve Physiology by Dr. RoomiDokumen12 halaman3rd Lecture On Nerve Physiology by Dr. RoomiMudassar RoomiBelum ada peringkat
- Cardiovascular Physiology 4 - Gomez MD PDFDokumen65 halamanCardiovascular Physiology 4 - Gomez MD PDFMelissa SalayogBelum ada peringkat
- Glomerular DiseaseDokumen98 halamanGlomerular DiseasePatrick TumewuBelum ada peringkat
- Laboratory Approach To AnemiasDokumen23 halamanLaboratory Approach To AnemiasDr. Ashish JawarkarBelum ada peringkat
- New Initial Management in TraumaDokumen69 halamanNew Initial Management in TraumaAhsan KhanBelum ada peringkat
- Macrocytic AnemiasDokumen28 halamanMacrocytic AnemiasDeepankar SrigyanBelum ada peringkat
- HIV-associated Nephropathies: Epidemiology, Pathology, Mechanisms and TreatmentDokumen11 halamanHIV-associated Nephropathies: Epidemiology, Pathology, Mechanisms and Treatmentsavitagera100% (1)
- Microcirculation as Related to ShockDari EverandMicrocirculation as Related to ShockDavid SheproBelum ada peringkat
- A Simple Guide to Platelet Disorders, Diagnosis, Treatment and Related ConditionsDari EverandA Simple Guide to Platelet Disorders, Diagnosis, Treatment and Related ConditionsBelum ada peringkat
- Biology AssignmentDokumen3 halamanBiology AssignmentAnny AlvrzBelum ada peringkat
- How To Beautify and Maintain Your Garden in The Power of The Holy SpiritDokumen28 halamanHow To Beautify and Maintain Your Garden in The Power of The Holy SpiritAnny AlvrzBelum ada peringkat
- Topic Breakdown 2nd Year First SemDokumen6 halamanTopic Breakdown 2nd Year First SemAnny AlvrzBelum ada peringkat
- Prepare For The End Time Move of The Holy Spirit Jesus Is Coming Again Apostle Abraham JCBC 101415Dokumen57 halamanPrepare For The End Time Move of The Holy Spirit Jesus Is Coming Again Apostle Abraham JCBC 101415Anny AlvrzBelum ada peringkat
- Build Your Garden To Be A Witness of God's FaithfulnessDokumen18 halamanBuild Your Garden To Be A Witness of God's FaithfulnessAnny AlvrzBelum ada peringkat
- Biofemme ICONDokumen34 halamanBiofemme ICONAnny AlvrzBelum ada peringkat
- Development of The Face 2015 PDFDokumen2 halamanDevelopment of The Face 2015 PDFAnny AlvrzBelum ada peringkat
- Histology of Ear and EyeDokumen2 halamanHistology of Ear and EyeAnny AlvrzBelum ada peringkat
- Ears and EyesDokumen4 halamanEars and EyesAnny AlvrzBelum ada peringkat
- Antibiotic StewardshipDokumen63 halamanAntibiotic StewardshipAnny AlvrzBelum ada peringkat
- Optimizing and Maximizing Antibiotic TherapyDokumen76 halamanOptimizing and Maximizing Antibiotic TherapyAnny AlvrzBelum ada peringkat
- Believe Signs and Wonders and MiraclesDokumen12 halamanBelieve Signs and Wonders and MiraclesAnny AlvrzBelum ada peringkat
- Cranial Nerves and Their Sensory Association NeuronsDokumen3 halamanCranial Nerves and Their Sensory Association NeuronsAnny AlvrzBelum ada peringkat
- Utilizing PKPD To Optimize TherapyDokumen39 halamanUtilizing PKPD To Optimize TherapyAnny AlvrzBelum ada peringkat
- Obedience Is The Key To Unlock Your MiraclesDokumen11 halamanObedience Is The Key To Unlock Your MiraclesAnny AlvrzBelum ada peringkat
- You Have The Power To Believe SignsDokumen18 halamanYou Have The Power To Believe SignsAnny AlvrzBelum ada peringkat
- Four Principles Approach To EthicsDokumen5 halamanFour Principles Approach To EthicsAnny AlvrzBelum ada peringkat
- Love Your GardenDokumen17 halamanLove Your GardenAnny AlvrzBelum ada peringkat
- Scalp Gross AnatomyDokumen5 halamanScalp Gross AnatomyAnny AlvrzBelum ada peringkat
- You Can Be VictoriousDokumen1 halamanYou Can Be VictoriousAnny AlvrzBelum ada peringkat
- (BiochemB) Signal Transduction - Dr. Viliran (Bernabe and Dela Rosa) PDFDokumen13 halaman(BiochemB) Signal Transduction - Dr. Viliran (Bernabe and Dela Rosa) PDFAnny AlvrzBelum ada peringkat
- You Are Not A FailureDokumen17 halamanYou Are Not A FailureAnny AlvrzBelum ada peringkat
- Autonomy & JusticeDokumen4 halamanAutonomy & JusticeAnny AlvrzBelum ada peringkat
- CSF and Ventricular SystemDokumen24 halamanCSF and Ventricular SystemAnny AlvrzBelum ada peringkat
- CFM I Physical Activity GuicoDokumen7 halamanCFM I Physical Activity GuicoAnny AlvrzBelum ada peringkat
- Filipino Family: Marthony P. Basco, MD, MPH DCFM - Feu, NRMFDokumen10 halamanFilipino Family: Marthony P. Basco, MD, MPH DCFM - Feu, NRMFAnny AlvrzBelum ada peringkat
- Waste Management: Louricha A. Opina-Tan, MD Department of Community and Family MedicineDokumen34 halamanWaste Management: Louricha A. Opina-Tan, MD Department of Community and Family MedicineAnny AlvrzBelum ada peringkat
- Anterior and Posterio Pituitary GlandDokumen7 halamanAnterior and Posterio Pituitary GlandAnny AlvrzBelum ada peringkat
- Tools in Family AssessmentDokumen3 halamanTools in Family AssessmentAnny Alvrz83% (6)
- Physio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionDokumen5 halamanPhysio B 1.2 Renal Physiology Pt. 4 (Dr. Vila) : Because of Increase Water ReabsorptionAnny AlvrzBelum ada peringkat
- Animals Lapbook COLORDokumen7 halamanAnimals Lapbook COLORIrynaBelum ada peringkat
- Cytology 3 ReportDokumen93 halamanCytology 3 ReportMoganambikai RagavanBelum ada peringkat
- Müller Gerd, Evo-Devo - Extending The Evolutionary Synthesis PDFDokumen7 halamanMüller Gerd, Evo-Devo - Extending The Evolutionary Synthesis PDFAristide de BésureBelum ada peringkat
- CellDokumen12 halamanCellMasTura MdZinBelum ada peringkat
- Animals ExerciseDokumen4 halamanAnimals ExerciseSabina ComanBelum ada peringkat
- Early DevelopmentDokumen2 halamanEarly DevelopmentyelloweverglowBelum ada peringkat
- DPP 1 Evolution Introduction AksDokumen2 halamanDPP 1 Evolution Introduction AksRia SriBelum ada peringkat
- NMAT BIOLOGY MOCK EXAM REVIEWDokumen7 halamanNMAT BIOLOGY MOCK EXAM REVIEWMDreamerBelum ada peringkat
- Spider Predation on Centipede Species in ChileDokumen2 halamanSpider Predation on Centipede Species in ChileHalisa IndrianiBelum ada peringkat
- Self Revision AnswerDokumen22 halamanSelf Revision AnswersaratvegaBelum ada peringkat
- Wildlife Fact File - Birds - Pgs. 251-260Dokumen20 halamanWildlife Fact File - Birds - Pgs. 251-260ClearMind84100% (2)
- TEMPORALIS MUSCLE FLAP RECONSTRUCTIONDokumen5 halamanTEMPORALIS MUSCLE FLAP RECONSTRUCTIONashajangamBelum ada peringkat
- Phylum Protozoa Classification: Elementary IdeaDokumen3 halamanPhylum Protozoa Classification: Elementary IdeaSudesh RathodBelum ada peringkat
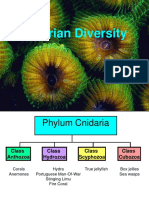
- 006 Cnidarian DiversityDokumen32 halaman006 Cnidarian DiversitydebasisBelum ada peringkat
- 336 1999 enDokumen6 halaman336 1999 enErvin TotiBelum ada peringkat
- Phylum CnidariaDokumen26 halamanPhylum CnidariaAbby SangualBelum ada peringkat
- New Species of "Tiger-Milk" Mushroom in Malaysia, Named As Lignosus TigerusDokumen7 halamanNew Species of "Tiger-Milk" Mushroom in Malaysia, Named As Lignosus TigerusLignosus RhinocerusBelum ada peringkat
- The Sliding Filament TheoryDokumen4 halamanThe Sliding Filament TheoryJinno VeldadBelum ada peringkat
- MutualismDokumen2 halamanMutualismJose Gregorio SuterBelum ada peringkat
- Evolution of KidneyDokumen127 halamanEvolution of Kidneyanon_9692255300% (1)
- Study of Cell WallDokumen42 halamanStudy of Cell WallWindy Lou BagayBelum ada peringkat
- Extraction,: Ancient DNA: Characterization, Molecular Cloning, and Enzymatic AmplificationDokumen5 halamanExtraction,: Ancient DNA: Characterization, Molecular Cloning, and Enzymatic AmplificationSara MagoBelum ada peringkat
- Homo Erectus Walks Amongst UsDokumen420 halamanHomo Erectus Walks Amongst Usheuristic25% (4)
- Student Homework on Reading Comprehension and ConnectorsDokumen52 halamanStudent Homework on Reading Comprehension and ConnectorsJohanZafiro 123Belum ada peringkat
- Names For Trace Fossils A Uniform Approa PDFDokumen22 halamanNames For Trace Fossils A Uniform Approa PDFcatfoulkrodBelum ada peringkat
- Dragonflies and Damselflies of MaltaDokumen123 halamanDragonflies and Damselflies of MaltaRam LeeBelum ada peringkat
- Taxonomic Study of The Family Scoliidae (Hymenoptera Aculeata) in IraqDokumen15 halamanTaxonomic Study of The Family Scoliidae (Hymenoptera Aculeata) in IraqInternational Network For Natural SciencesBelum ada peringkat
- Sanitary DefectsDokumen1 halamanSanitary DefectsJzj Mi SanMateo Isabela67% (3)
- Biology Chapter 2 Kingdom Classification Unint 2 AnamaliDokumen14 halamanBiology Chapter 2 Kingdom Classification Unint 2 AnamaliJaya SinghBelum ada peringkat
- Alert !: Pinning and Labeling InsectsDokumen4 halamanAlert !: Pinning and Labeling InsectsUlises Infante HuaytallaBelum ada peringkat