Anda mungkin juga menyukai
- Jurnal Play Therapy in Turkey PDFDokumen5 halamanJurnal Play Therapy in Turkey PDFwilmaBelum ada peringkat
- Clinical Features and Resolution of Food Protein-Induced Enterocolitis Syndrome: 10-Year ExperienceDokumen12 halamanClinical Features and Resolution of Food Protein-Induced Enterocolitis Syndrome: 10-Year ExperiencewilmaBelum ada peringkat
- 1 s2.0 S009167491301909X Main PDFDokumen9 halaman1 s2.0 S009167491301909X Main PDFwilmaBelum ada peringkat
- Initial Resuscitation and Stabilization of The Periviable Neonate: The Golden-Hour ApproachDokumen5 halamanInitial Resuscitation and Stabilization of The Periviable Neonate: The Golden-Hour ApproachwilmaBelum ada peringkat
- Pharyngeal Swallowing: Defining Pharyngeal and Upper Esophageal Sphincter Relationships in Human NeonatesDokumen7 halamanPharyngeal Swallowing: Defining Pharyngeal and Upper Esophageal Sphincter Relationships in Human NeonateswilmaBelum ada peringkat
- Fat Cell Size, Insulin Sensitivity, and Inflammation in Obese ChildrenDokumen6 halamanFat Cell Size, Insulin Sensitivity, and Inflammation in Obese ChildrenwilmaBelum ada peringkat
- Advanced Life Support Training and Assessment PDFDokumen6 halamanAdvanced Life Support Training and Assessment PDFwilmaBelum ada peringkat
- Basic Trauma Life Support For Firefigbters PDFDokumen1 halamanBasic Trauma Life Support For Firefigbters PDFwilmaBelum ada peringkat
- Teaching and Teacher Education: Josepha A. Blay, Judith IresonDokumen12 halamanTeaching and Teacher Education: Josepha A. Blay, Judith IresonwilmaBelum ada peringkat
- 43 PDFDokumen9 halaman43 PDFwilmaBelum ada peringkat
- Applied Nursing ResearchDokumen5 halamanApplied Nursing ResearchwilmaBelum ada peringkat
- Vitamin D Insufficiency Is Associated With Challenge-Proven Food Allergy in InfantsDokumen14 halamanVitamin D Insufficiency Is Associated With Challenge-Proven Food Allergy in InfantswilmaBelum ada peringkat
- S0196064413X00125 S0196064413010895 Main PDFDokumen2 halamanS0196064413X00125 S0196064413010895 Main PDFwilmaBelum ada peringkat
- 1 s2.0 S0145213414000416 MainDokumen8 halaman1 s2.0 S0145213414000416 MainwilmaBelum ada peringkat
- 1 s2.0 S0264410X14000085 Main PDFDokumen8 halaman1 s2.0 S0264410X14000085 Main PDFwilmaBelum ada peringkat
- 1 s2.0 S027153179800027X Main PDFDokumen29 halaman1 s2.0 S027153179800027X Main PDFwilmaBelum ada peringkat
- Visually Transformingartworkandguidedimageryasawaytoreduce PDFDokumen4 halamanVisually Transformingartworkandguidedimageryasawaytoreduce PDFwilmaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Reading AssignmentDokumen15 halamanReading AssignmentHazel AbayaBelum ada peringkat
- Municipal Nutrition Action Plan 2023 2025 Ver2Dokumen44 halamanMunicipal Nutrition Action Plan 2023 2025 Ver2Timothy Custodio100% (2)
- Tor LGCB Asr Moha 14 FebDokumen16 halamanTor LGCB Asr Moha 14 Febkilli00wearBelum ada peringkat
- Sagaing Region Profile FinalDokumen4 halamanSagaing Region Profile FinalThet Ko KoBelum ada peringkat
- 12.14 - Paparan DUNCNN - Debora Comini From UnicefDokumen11 halaman12.14 - Paparan DUNCNN - Debora Comini From Unicefveny AfreBelum ada peringkat
- Strategies of Reducing Malnutrition by Caregivers Amongst Children 0-5 Years in Opiro CommunityDokumen8 halamanStrategies of Reducing Malnutrition by Caregivers Amongst Children 0-5 Years in Opiro CommunityEgbuna ChukwuebukaBelum ada peringkat
- RAKOTOMALALA, Bodo, Case Study Under The Social Sector Public Expenditure Review - 2014, Antananarivo: UNICEF Madagascar, 2014, 117 P.Dokumen118 halamanRAKOTOMALALA, Bodo, Case Study Under The Social Sector Public Expenditure Review - 2014, Antananarivo: UNICEF Madagascar, 2014, 117 P.HayZara MadagascarBelum ada peringkat
- Abdi Seminar On Updates of SAMDokumen74 halamanAbdi Seminar On Updates of SAMAbdi KebedeBelum ada peringkat
- Nutrition in The First 1000 DaysDokumen7 halamanNutrition in The First 1000 DaysYoki VirgoBelum ada peringkat
- 29729-Article Text-122972-1-10-20201231 - Keragaman PanganDokumen7 halaman29729-Article Text-122972-1-10-20201231 - Keragaman Pangans_ton77Belum ada peringkat
- CFLGA Handbook - Section On Assessment CriteriaDokumen25 halamanCFLGA Handbook - Section On Assessment CriteriaJim100% (6)
- Primer Atlas Mundial de La Obesidad Infantil.Dokumen212 halamanPrimer Atlas Mundial de La Obesidad Infantil.Cooperativa.clBelum ada peringkat
- 2 - Determinants of Acute Malnutrition Among Children Aged 6-59 Months Visiting Public Health Facilities in Gambella Town, Southwest Ethiopia Unmatched Case-Control StudyDokumen10 halaman2 - Determinants of Acute Malnutrition Among Children Aged 6-59 Months Visiting Public Health Facilities in Gambella Town, Southwest Ethiopia Unmatched Case-Control StudyRezki Purnama YusufBelum ada peringkat
- Reports and OrganisationsDokumen13 halamanReports and Organisationsvinita thakurBelum ada peringkat
- Literature Review Penatalaksanaan Kasus Stunting Pada BalitaDokumen11 halamanLiterature Review Penatalaksanaan Kasus Stunting Pada Balitamaulana ekaBelum ada peringkat
- ECD Best Practices PDFDokumen60 halamanECD Best Practices PDFJasiz Philipe OmbuguBelum ada peringkat
- A Study of Exclusive Breastfeeding and Its Impact On Nutritional Status of Child in EAG StatesDokumen21 halamanA Study of Exclusive Breastfeeding and Its Impact On Nutritional Status of Child in EAG StatessiskaBelum ada peringkat
- Health EducationDokumen7 halamanHealth EducationRhu LibonBelum ada peringkat
- Stunting and Poverty in IndonesiaDokumen3 halamanStunting and Poverty in IndonesiaDIVA PATRICIA MARSHABelum ada peringkat
- Mejía Acosta and Haddad2014The Politics of Success in The Fight Against Malnutrition in PeruDokumen10 halamanMejía Acosta and Haddad2014The Politics of Success in The Fight Against Malnutrition in PeruPWaaaaBelum ada peringkat
- 4 P'sDokumen23 halaman4 P'sMeetch Soriano100% (1)
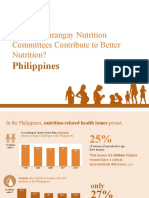
- How Do Barangay Nutrition Committees Contribute To Better Nutrition?Dokumen20 halamanHow Do Barangay Nutrition Committees Contribute To Better Nutrition?Angelito CortunaBelum ada peringkat
- 2020 Highlights From The Nutrition Guidelines For Cystic Fibrosis in Australia and New ZealandDokumen10 halaman2020 Highlights From The Nutrition Guidelines For Cystic Fibrosis in Australia and New ZealandMaria Paula CastroBelum ada peringkat
- Prevalence of Undernutrition Among Musahar Children Aged Between 12 To 59 Months in Urban Siraha District, NepalDokumen8 halamanPrevalence of Undernutrition Among Musahar Children Aged Between 12 To 59 Months in Urban Siraha District, NepalMan Bahadur LamaBelum ada peringkat
- 1 s2.0 S2666149722000202 MainDokumen6 halaman1 s2.0 S2666149722000202 MainALEXANDRE SOUSABelum ada peringkat
- Autonutrition Status Program Version 5.2Dokumen9 halamanAutonutrition Status Program Version 5.2Racel FuentesBelum ada peringkat
- PDGKIDokumen76 halamanPDGKIhayinarsihBelum ada peringkat
- NRC Guidelines GujrathDokumen68 halamanNRC Guidelines GujrathNirajkumar KondekarBelum ada peringkat
- Thesis Recent With Interp AmrsDokumen62 halamanThesis Recent With Interp AmrsAira AmorosoBelum ada peringkat
- Moringa (Moringa Oleifera) Flour in Wet Noodles As: Fortification of Porang (Amorphophallus Muelleri) andDokumen7 halamanMoringa (Moringa Oleifera) Flour in Wet Noodles As: Fortification of Porang (Amorphophallus Muelleri) andaskasBelum ada peringkat