Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Smoking N CariesDokumen59 halamanSmoking N CariesdigdouwBelum ada peringkat
- Polyurethane SDokumen7 halamanPolyurethane SdigdouwBelum ada peringkat
- Eaat 14 I 1 P 149Dokumen9 halamanEaat 14 I 1 P 149digdouwBelum ada peringkat
- 0103 6440 BDJ 26 04 00347Dokumen4 halaman0103 6440 BDJ 26 04 00347digdouwBelum ada peringkat
- Naumann 2009Dokumen14 halamanNaumann 2009digdouwBelum ada peringkat
- JEORDokumen6 halamanJEORdigdouwBelum ada peringkat
- Apical Sealing Ability of Four Different Root Canal Sealers An in Vitro StudyDokumen5 halamanApical Sealing Ability of Four Different Root Canal Sealers An in Vitro StudydigdouwBelum ada peringkat
- Daftar PustakaDokumen3 halamanDaftar PustakadigdouwBelum ada peringkat
- Removal of Calcium HydroxideDokumen7 halamanRemoval of Calcium HydroxidedigdouwBelum ada peringkat
- Fisher Et Al-2009-Journal of Applied MicrobiologyDokumen7 halamanFisher Et Al-2009-Journal of Applied MicrobiologydigdouwBelum ada peringkat
- Walkeretal ProDokumen7 halamanWalkeretal ProdigdouwBelum ada peringkat
- Jurnal RANKLDokumen10 halamanJurnal RANKLdigdouwBelum ada peringkat
- Calcium Hydroxide Dressing and Periapical RepairDokumen6 halamanCalcium Hydroxide Dressing and Periapical RepairdigdouwBelum ada peringkat
- Jurnal 6 Tugas DRG Irlen 303Dokumen3 halamanJurnal 6 Tugas DRG Irlen 303digdouwBelum ada peringkat
- DAFTAR PUSTAKAaaaaaaDokumen2 halamanDAFTAR PUSTAKAaaaaaadigdouwBelum ada peringkat
- Iis ManisDokumen6 halamanIis ManisNurbaetty RochmahBelum ada peringkat
- Root Resorption Associated With Orthodontic Force in IL-1B Knockout MouseDokumen3 halamanRoot Resorption Associated With Orthodontic Force in IL-1B Knockout MousedigdouwBelum ada peringkat
- Jurnal 5 Tugas DRG Irlen 303Dokumen6 halamanJurnal 5 Tugas DRG Irlen 303digdouwBelum ada peringkat
- Polyurethane SDokumen7 halamanPolyurethane SdigdouwBelum ada peringkat
- Ebd 305Dokumen5 halamanEbd 305digdouwBelum ada peringkat
- DocumentDokumen22 halamanDocumentdigdouwBelum ada peringkat
- Study of The Ablative Effects of Nd:YAG or Er:YAG Laser RadiationDokumen3 halamanStudy of The Ablative Effects of Nd:YAG or Er:YAG Laser RadiationdigdouwBelum ada peringkat
- Effect of Er:Yag Laser Irradiation On Enamel Caries PreventionDokumen5 halamanEffect of Er:Yag Laser Irradiation On Enamel Caries PreventiondigdouwBelum ada peringkat
- Review - AJD June 2006Dokumen9 halamanReview - AJD June 2006digdouwBelum ada peringkat
- Prevention of Caries by Pulsed CO, Laser Pre-Treatment of Enamel: An In-Vitro StudyDokumen5 halamanPrevention of Caries by Pulsed CO, Laser Pre-Treatment of Enamel: An In-Vitro StudydigdouwBelum ada peringkat
- Review - AJD June 2006Dokumen9 halamanReview - AJD June 2006digdouwBelum ada peringkat
- Prevention of Caries by Pulsed CO, Laser Pre-Treatment of Enamel: An In-Vitro StudyDokumen5 halamanPrevention of Caries by Pulsed CO, Laser Pre-Treatment of Enamel: An In-Vitro StudydigdouwBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- MoxiquinDokumen50 halamanMoxiquinpabitraBelum ada peringkat
- CoppDokumen1 halamanCoppEze Nicholas Ude0% (1)
- List of Illegal Products Found 2014 ONE PAGERDokumen1 halamanList of Illegal Products Found 2014 ONE PAGERAkash GuptaBelum ada peringkat
- Flow Through Cell Dissolution ApparatusDokumen22 halamanFlow Through Cell Dissolution ApparatusKimberly MccoyBelum ada peringkat
- DeclomycineDokumen14 halamanDeclomycineRamanasarmaBelum ada peringkat
- Chapter 4: PsychopharmacologyDokumen37 halamanChapter 4: PsychopharmacologyGummyCola100% (2)
- Preoperative Testing and Medication ManagementDokumen27 halamanPreoperative Testing and Medication ManagementWidya JelitaBelum ada peringkat
- Animal Testing Essential To Medical ProgressDokumen7 halamanAnimal Testing Essential To Medical ProgressLayalBelum ada peringkat
- Drusadg Study For Paracetamol Omeprazole and Vitamin B ComplexDokumen3 halamanDrusadg Study For Paracetamol Omeprazole and Vitamin B ComplexzerpthederpBelum ada peringkat
- Introduction To Clinical TrialsDokumen9 halamanIntroduction To Clinical Trialsmuhammad murtazaBelum ada peringkat
- Procedure To Insert An IV DripDokumen5 halamanProcedure To Insert An IV DripanggiBelum ada peringkat
- Lipitor: (Atorvastatin Calcium) TabletsDokumen29 halamanLipitor: (Atorvastatin Calcium) TabletsEvelinaĐulbićBelum ada peringkat
- Characterization of Adsorption Behavior by Solid Dosage Form Excipients in Formulation DevelopmentDokumen8 halamanCharacterization of Adsorption Behavior by Solid Dosage Form Excipients in Formulation DevelopmentKietBelum ada peringkat
- Substance List Dec10Dokumen25 halamanSubstance List Dec10Ricki_Ogston_4896Belum ada peringkat
- Pharmacuetical Microbiology Manual 2014 PDFDokumen86 halamanPharmacuetical Microbiology Manual 2014 PDFteaBelum ada peringkat
- No Hipertensi Harga (RP) PaketDokumen2 halamanNo Hipertensi Harga (RP) PaketVania Azalia HariyantoBelum ada peringkat
- Adi CholDokumen4 halamanAdi CholIqbal MaulanaBelum ada peringkat
- Organizational BehavioreDokumen8 halamanOrganizational Behavioresss1104Belum ada peringkat
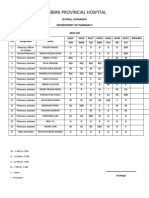
- Lumbini Provincial Hospital: Department of PharmacyDokumen2 halamanLumbini Provincial Hospital: Department of PharmacyImdadHussainOPositiveBelum ada peringkat
- US6132758Dokumen6 halamanUS6132758Okta Dewi PermatasariBelum ada peringkat
- Pharmacological Interactions of VasoconstrictorsDokumen8 halamanPharmacological Interactions of VasoconstrictorsValeska Farina EspinosaBelum ada peringkat
- By:-Devang Gangwani and Ashish Juriani - Final Year Bpharm (2018)Dokumen20 halamanBy:-Devang Gangwani and Ashish Juriani - Final Year Bpharm (2018)Devang GangwaniBelum ada peringkat
- Perry's Chemical Engineers' Handbook, 8th Edition 242Dokumen1 halamanPerry's Chemical Engineers' Handbook, 8th Edition 242Ooi Chia EnBelum ada peringkat
- A Comparison of Hemodynamic Changes During Laryngoscopy and Endotracheal Intubation by Using Three Modalities of Anesthesia InductionDokumen5 halamanA Comparison of Hemodynamic Changes During Laryngoscopy and Endotracheal Intubation by Using Three Modalities of Anesthesia Inductionammaa_Belum ada peringkat
- Food-Drug InteractionsDokumen5 halamanFood-Drug InteractionsDwi SrijonoBelum ada peringkat
- Eris Healthcare GX Price ListDokumen9 halamanEris Healthcare GX Price ListPalakBelum ada peringkat
- Opioids Vs Nonopioids For Chronic Back, Hip, or Knee PainDokumen4 halamanOpioids Vs Nonopioids For Chronic Back, Hip, or Knee PainMarco Antonio KoffBelum ada peringkat
- Eur J Hosp Pharm 2015 Humbert Delaloye 56 8 FurosemidDokumen4 halamanEur J Hosp Pharm 2015 Humbert Delaloye 56 8 FurosemidChemayanti SurbaktiBelum ada peringkat
- Philhealth Cf4 2017-2018Dokumen8 halamanPhilhealth Cf4 2017-2018Julius Yves Dulfo BagacayBelum ada peringkat
- VivaSante - CorporationDokumen15 halamanVivaSante - CorporationFranz OrtegaBelum ada peringkat