Anda mungkin juga menyukai
- Eggs and Beyond: Is Dietary Cholesterol No Longer Important?Dokumen2 halamanEggs and Beyond: Is Dietary Cholesterol No Longer Important?Dianne Faye ManabatBelum ada peringkat
- Reconsidering The Importance of The Association of Egg Consumption and Dietary Cholesterol With Cardiovascular Disease RiskDokumen2 halamanReconsidering The Importance of The Association of Egg Consumption and Dietary Cholesterol With Cardiovascular Disease RiskFernandoBelum ada peringkat
- Busting The Myth of Saturated Fat in Heart Disease British Medical Journal 2013Dokumen2 halamanBusting The Myth of Saturated Fat in Heart Disease British Medical Journal 2013jackjensen2852Belum ada peringkat
- Dietary Cholesterol and Atherosclerosis: ReviewDokumen11 halamanDietary Cholesterol and Atherosclerosis: ReviewRurin WidaBelum ada peringkat
- Where Do Eggs Fit in A Heart-Healthy DietDokumen6 halamanWhere Do Eggs Fit in A Heart-Healthy DietPier Paolo Dal MonteBelum ada peringkat
- Atherosclerosis Is A Disease in Which Plaque Builds Up Inside Your Arterie, Plaque Is Basically Build ofDokumen12 halamanAtherosclerosis Is A Disease in Which Plaque Builds Up Inside Your Arterie, Plaque Is Basically Build ofadam zosmaBelum ada peringkat
- Diet Heart MythDokumen23 halamanDiet Heart MythΚυριακίδης ΚώσταςBelum ada peringkat
- Nutrition PDFDokumen2 halamanNutrition PDFCamila BonillaBelum ada peringkat
- Andrew Maxwell, M.D.: From: Sent: To: SubjectDokumen4 halamanAndrew Maxwell, M.D.: From: Sent: To: SubjectHeart of the Valley, Pediatric CardiologyBelum ada peringkat
- Protein intake and atherosclerosisDokumen7 halamanProtein intake and atherosclerosisnouval_iqbalBelum ada peringkat
- Types of Dietary Fat and Risk of Coronary Heart Disease: A Critical ReviewDokumen15 halamanTypes of Dietary Fat and Risk of Coronary Heart Disease: A Critical ReviewMegan KnightBelum ada peringkat
- Hypercholesterolemia Among Children: When Is It High, and When Is It Really High?Dokumen4 halamanHypercholesterolemia Among Children: When Is It High, and When Is It Really High?Brenda CaraveoBelum ada peringkat
- Lipid Screen PedsDokumen13 halamanLipid Screen PedsEnerolisa ParedesBelum ada peringkat
- Stroke.: Nutrition and Stroke PreventionDokumen7 halamanStroke.: Nutrition and Stroke Preventionrandey92Belum ada peringkat
- Egg Consumption in Relation To Cardiovascular Disease and Mortality: The Physicians' Health StudyDokumen6 halamanEgg Consumption in Relation To Cardiovascular Disease and Mortality: The Physicians' Health Studykrazyj123Belum ada peringkat
- Polygenic Hypercholesterolemia: Causes, Risks & TreatmentDokumen6 halamanPolygenic Hypercholesterolemia: Causes, Risks & TreatmentSamhitha Ayurvedic ChennaiBelum ada peringkat
- Background:: ConclusionDokumen2 halamanBackground:: ConclusionMounica PaturuBelum ada peringkat
- ANNALS DyslipidemiaDokumen16 halamanANNALS Dyslipidemiaewb100% (1)
- What Is The Ideal Cholesterol Level by Joel Fuhrman MDDokumen4 halamanWhat Is The Ideal Cholesterol Level by Joel Fuhrman MDDrRod SmithBelum ada peringkat
- Management of HyperlipidemiaDokumen34 halamanManagement of HyperlipidemiaCarleta StanBelum ada peringkat
- A Plant-Based Diet and StrokeDokumen1 halamanA Plant-Based Diet and Strokemastergunner99Belum ada peringkat
- Alternatives To Low-Fat DietsDokumen2 halamanAlternatives To Low-Fat DietsWidi QdiwBelum ada peringkat
- A Prospective Study of Egg Consumption and Risk of Cardiovascular Disease in Men and WomenDokumen8 halamanA Prospective Study of Egg Consumption and Risk of Cardiovascular Disease in Men and Womenkrazyj123Belum ada peringkat
- 7.systematic Review and Meta-Analysis of Clinical Trials of The Effects of Low Carbohydrate Diets On Cardiovascular Risk Factors.Dokumen19 halaman7.systematic Review and Meta-Analysis of Clinical Trials of The Effects of Low Carbohydrate Diets On Cardiovascular Risk Factors.Ambar Sofía MieresBelum ada peringkat
- AHA Advisory OKs Eating Cholesterol in ModerationDokumen3 halamanAHA Advisory OKs Eating Cholesterol in ModerationGerry FonziBelum ada peringkat
- Literature Review AhnDokumen9 halamanLiterature Review Ahnapi-302130624Belum ada peringkat
- 8731 Ch02Dokumen51 halaman8731 Ch02Mohammed Salim AmmorBelum ada peringkat
- Chapter 1Dokumen8 halamanChapter 1Mirabete Kurt marvin - FHC1Belum ada peringkat
- New Evidence Shows Satuared Fats Are Heart HealthyDokumen5 halamanNew Evidence Shows Satuared Fats Are Heart Healthyapi-296456392Belum ada peringkat
- Nutrients: Egg Intake in Chronic Kidney DiseaseDokumen13 halamanNutrients: Egg Intake in Chronic Kidney DiseaseAzzahra Nur FadhilahBelum ada peringkat
- Stoke NutritionDokumen14 halamanStoke Nutritionapi-150223943Belum ada peringkat
- Heart Disease and Stroke Scientific ReviewDokumen6 halamanHeart Disease and Stroke Scientific Reviewapi-371380624Belum ada peringkat
- Siri-Tarino - Saturated Fat CHO e DCVDokumen8 halamanSiri-Tarino - Saturated Fat CHO e DCVGracielaRecheBelum ada peringkat
- Meta-analysis finds no link between saturated fat intake and cardiovascular disease riskDokumen31 halamanMeta-analysis finds no link between saturated fat intake and cardiovascular disease riskMozHeartBelum ada peringkat
- Hypertension 2012 West 58 63Dokumen7 halamanHypertension 2012 West 58 63Rully SyahrizalBelum ada peringkat
- Chapter 2 - Grade 12 He3 (Setb Backsub)Dokumen6 halamanChapter 2 - Grade 12 He3 (Setb Backsub)Mirabete Kurt marvin - FHC1Belum ada peringkat
- Risk Factors for Heart Disease Among Female University StudentsDokumen6 halamanRisk Factors for Heart Disease Among Female University StudentsMuhammad Irfan JamilBelum ada peringkat
- Dislipidemia in PregnancyDokumen7 halamanDislipidemia in PregnancyandreaBelum ada peringkat
- Debunking The Myth About High Cholesterol LevelsDokumen5 halamanDebunking The Myth About High Cholesterol LevelsmacdaveBelum ada peringkat
- 7 Simple Ways To Avoid CancerDokumen4 halaman7 Simple Ways To Avoid CancerjohntandraBelum ada peringkat
- Basic Science Pathophysiology: The Cardiorenal Metabolic SyndromeDokumen3 halamanBasic Science Pathophysiology: The Cardiorenal Metabolic Syndromefilema2000Belum ada peringkat
- Nej M 199504133321512Dokumen7 halamanNej M 199504133321512Sylvia IngridBelum ada peringkat
- Pres 3Dokumen25 halamanPres 3api-262185461Belum ada peringkat
- Diet and HealthDokumen4 halamanDiet and HealthR VBelum ada peringkat
- High Cholesterol Research PaperDokumen5 halamanHigh Cholesterol Research Papergz8aqe8w100% (1)
- Dietary Cholesterol's Impact on LDL and HDL RatiosDokumen9 halamanDietary Cholesterol's Impact on LDL and HDL RatiosTyrone PenningBelum ada peringkat
- Hypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionDari EverandHypoglycemia in Diabetes: Pathophysiology, Prevalence, and PreventionBelum ada peringkat
- GrasasDokumen12 halamanGrasasCristian Camilo SaavedraBelum ada peringkat
- Egg consumption and heart health: A review summarizes risksDokumen7 halamanEgg consumption and heart health: A review summarizes risksLucas BarbosaBelum ada peringkat
- Nutrition and HypertensionDokumen3 halamanNutrition and HypertensionKajee GrantBelum ada peringkat
- More Bad News For SugarDokumen2 halamanMore Bad News For SugarJunita Putri SimorangkirBelum ada peringkat
- The Truth About Eating EggsDokumen7 halamanThe Truth About Eating Eggsale.123Belum ada peringkat
- Obesity and CV OutcomesDokumen19 halamanObesity and CV OutcomesLivia Maria RaduBelum ada peringkat
- Dietary fat recommendations wrong, based on zero evidenceDokumen4 halamanDietary fat recommendations wrong, based on zero evidenceperete69Belum ada peringkat
- Obesity and CVDDokumen19 halamanObesity and CVDAnindira RustandiBelum ada peringkat
- Dietary Recommendations For Familial HypercholestDokumen3 halamanDietary Recommendations For Familial HypercholestMaria Luiza BarbosaBelum ada peringkat
- Background of The StudyDokumen10 halamanBackground of The StudyReimond VinceBelum ada peringkat
- Ahei & HeiDokumen12 halamanAhei & HeiBushra KainaatBelum ada peringkat
- Art Beneficios Del Huevo PDFDokumen13 halamanArt Beneficios Del Huevo PDFAldaveLuisBelum ada peringkat
- Plasma Lipids: Optimal Levels for HealthDari EverandPlasma Lipids: Optimal Levels for HealthAmerican Health FoundationBelum ada peringkat
- 187-Article Text-489-1-10-20210302Dokumen6 halaman187-Article Text-489-1-10-20210302Andri NugrahaBelum ada peringkat
- 44 217 1 PBDokumen5 halaman44 217 1 PBDes KinBelum ada peringkat
- Daftar PustakaDokumen2 halamanDaftar PustakaAndri NugrahaBelum ada peringkat
- Rational For Cholesterol PDFDokumen2 halamanRational For Cholesterol PDFAndri NugrahaBelum ada peringkat
- CPD + Uterine Rupture PDFDokumen50 halamanCPD + Uterine Rupture PDFAndri NugrahaBelum ada peringkat
- Question No EFSA-Q-2008-085Dokumen12 halamanQuestion No EFSA-Q-2008-085Andri NugrahaBelum ada peringkat
- Isa pp042 046 PDFDokumen5 halamanIsa pp042 046 PDFAndri NugrahaBelum ada peringkat
- Case Report: The Active Management of Impending Cephalopelvic Disproportion in Nulliparous Women at Term: A Case SeriesDokumen6 halamanCase Report: The Active Management of Impending Cephalopelvic Disproportion in Nulliparous Women at Term: A Case SeriesAnastasia FebriantiBelum ada peringkat
- Nutrition Support of Children With Chronic LiverDokumen14 halamanNutrition Support of Children With Chronic LiverMarcia SchneiderBelum ada peringkat
- Lipids: Fatty AcidsDokumen10 halamanLipids: Fatty AcidsRhealyn IliganBelum ada peringkat
- Lipid Metabolism and Health - EBOOKOID PDFDokumen377 halamanLipid Metabolism and Health - EBOOKOID PDFniluh suwasantiBelum ada peringkat
- A Review On Causes and Risk Factors of HyperlipidemiaDokumen6 halamanA Review On Causes and Risk Factors of HyperlipidemiaHam jungBelum ada peringkat
- Food and Chemical Toxicology: Beata Olas, Magdalena Bry SDokumen8 halamanFood and Chemical Toxicology: Beata Olas, Magdalena Bry Santonio escuderoBelum ada peringkat
- Rice: A Global Crop with Medicinal UsesDokumen17 halamanRice: A Global Crop with Medicinal UsesMohamad Saadatian SipanBelum ada peringkat
- The Effect of Cloud Ear FungusDokumen2 halamanThe Effect of Cloud Ear FungusElyza Joy RallosBelum ada peringkat
- Lipids and Lipoproteins: Characteristics, Functions, and MeasurementDokumen5 halamanLipids and Lipoproteins: Characteristics, Functions, and MeasurementMica BernardoBelum ada peringkat
- MBM Home Quiz BEFORE MIDTERMDokumen38 halamanMBM Home Quiz BEFORE MIDTERMbhagavan prasadBelum ada peringkat
- Turmeric Potential Health Benefits.9Dokumen13 halamanTurmeric Potential Health Benefits.9HandayaniBelum ada peringkat
- Effects of Dietary Chitosan On Serum Lipid and Lipoprotein Concentrations in RatsDokumen5 halamanEffects of Dietary Chitosan On Serum Lipid and Lipoprotein Concentrations in RatsEi Ei ThetBelum ada peringkat
- Evaluation of Medicinal Effects of Gynura Procumbens Leave Extracts On Oxidative Glycemic Lipidomics and Enzymatic ProfiDokumen7 halamanEvaluation of Medicinal Effects of Gynura Procumbens Leave Extracts On Oxidative Glycemic Lipidomics and Enzymatic Profimitu afrinBelum ada peringkat
- JENKINS, 1987 - Low-Glycemic Index Diet in Hyperlipidemia - Use of Traditional Starchy FoodsDokumen6 halamanJENKINS, 1987 - Low-Glycemic Index Diet in Hyperlipidemia - Use of Traditional Starchy FoodsAdrianoBelum ada peringkat
- Natural Homeopathic Remedies For High CholesterolDokumen54 halamanNatural Homeopathic Remedies For High Cholesterolssrkm guptaBelum ada peringkat
- Clinical Chemistry Mcqs Carbohydrates: RD THDokumen20 halamanClinical Chemistry Mcqs Carbohydrates: RD THJoyce Rosette Cabutotan Vergara67% (3)
- Cardiovascular Diseases Traditional and Non-TraditDokumen7 halamanCardiovascular Diseases Traditional and Non-TraditArham SheikhBelum ada peringkat
- Shana Sharma 8757100315Dokumen26 halamanShana Sharma 8757100315gaurav SharmaBelum ada peringkat
- Antihyperlipidemic Activity of Zygophyllum Simplex Ethanolic Extract On High Cholesterol Diet-Induced Hyperlipidemia in RatsDokumen18 halamanAntihyperlipidemic Activity of Zygophyllum Simplex Ethanolic Extract On High Cholesterol Diet-Induced Hyperlipidemia in Ratsأياد المشهدانيBelum ada peringkat
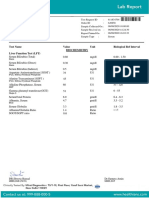
- Test Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Dokumen7 halamanTest Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Himanshu GarkhelBelum ada peringkat
- Laporan Hasil Penelitian Korelasi Rasio Kolesterol Total Terhadap HDL Dengan Prediksi Outcome Stroke Iskemik AkutDokumen13 halamanLaporan Hasil Penelitian Korelasi Rasio Kolesterol Total Terhadap HDL Dengan Prediksi Outcome Stroke Iskemik AkutRay HannaBelum ada peringkat
- Dietetic Technician, Registered Exam!: An All-Inclusive Guide To TheDokumen38 halamanDietetic Technician, Registered Exam!: An All-Inclusive Guide To TheAJ MendezBelum ada peringkat
- Assessment 1 unit 1: Cardiovascular Disease and Heart FunctionDokumen14 halamanAssessment 1 unit 1: Cardiovascular Disease and Heart Functionmaya 1DBelum ada peringkat
- Gamma-Oryzanol Benefits for Lipids & MenopauseDokumen10 halamanGamma-Oryzanol Benefits for Lipids & MenopauseSharif HossenBelum ada peringkat
- Dislipidemia Lancet Durrington PDFDokumen15 halamanDislipidemia Lancet Durrington PDFAlphaJulissa JuarezBelum ada peringkat
- Comprehensive Essay BiochemistryDokumen3 halamanComprehensive Essay BiochemistryFloreleneBelum ada peringkat
- Effects of Chili Pepper on Broiler Lipids and PerformanceDokumen7 halamanEffects of Chili Pepper on Broiler Lipids and PerformanceElena DamianBelum ada peringkat
- Carbohydrates-Lipids 1Dokumen6 halamanCarbohydrates-Lipids 1Michal VillanuevaBelum ada peringkat
- Nuno Nina CellWaterDokumen21 halamanNuno Nina CellWatershanti08100% (1)
- Cardiovascular Benefits and Risks of Moderate Alcohol ConsumptionDokumen26 halamanCardiovascular Benefits and Risks of Moderate Alcohol ConsumptionJessica BarcelonaBelum ada peringkat
- The Effect of Ginger (Zingiber Officinale) As An Ancient Medicinal Plant On Improving Blood LipidsDokumen5 halamanThe Effect of Ginger (Zingiber Officinale) As An Ancient Medicinal Plant On Improving Blood LipidsShania Astanti SimanjuntakBelum ada peringkat