Anda mungkin juga menyukai
- Diabetic Patients With Acute Coronary SyndromesDokumen6 halamanDiabetic Patients With Acute Coronary SyndromesMarnia SulfianaBelum ada peringkat
- Diabetes A Significant Contributor To ComplicationsDokumen9 halamanDiabetes A Significant Contributor To ComplicationsMarnia SulfianaBelum ada peringkat
- Official Score Certificate: Speaking WritingDokumen1 halamanOfficial Score Certificate: Speaking Writingsidiq16Belum ada peringkat
- Jurnal IkgmDokumen11 halamanJurnal IkgmMonika WerdiningsihBelum ada peringkat
- 1 s2.0 S1521690X0800170X MainDokumen14 halaman1 s2.0 S1521690X0800170X MainMarnia SulfianaBelum ada peringkat
- Wound HealingDokumen7 halamanWound HealingMarnia SulfianaBelum ada peringkat
- Journal of Asian Economics: Cassey Lee, Yoshifumi FukunagaDokumen15 halamanJournal of Asian Economics: Cassey Lee, Yoshifumi FukunagaMarnia SulfianaBelum ada peringkat
- Prontosan Askina Range Clinical and Scientific EvidenceDokumen60 halamanProntosan Askina Range Clinical and Scientific EvidenceMarnia SulfianaBelum ada peringkat
- Asean, EuDokumen21 halamanAsean, EuAnisur Rahman FaroqueBelum ada peringkat
- Wound HealingDokumen7 halamanWound HealingMarnia SulfianaBelum ada peringkat
- Sabin Et Al-2015-Journal of Paediatrics and Child HealthDokumen5 halamanSabin Et Al-2015-Journal of Paediatrics and Child HealthMarnia SulfianaBelum ada peringkat
- Distraction Techniques For Children Undergoing ProcedursDokumen30 halamanDistraction Techniques For Children Undergoing ProcedursMarnia SulfianaBelum ada peringkat
- Belimbing Dan MentimunDokumen11 halamanBelimbing Dan MentimunMarnia SulfianaBelum ada peringkat
- 1 s2.0 S0002870309007807 MainDokumen9 halaman1 s2.0 S0002870309007807 MainMarnia SulfianaBelum ada peringkat
- 1 s2.0 S1521690X08001711 MainDokumen18 halaman1 s2.0 S1521690X08001711 MainMarnia SulfianaBelum ada peringkat
- 1 s2.0 S2256208714001308 MainDokumen19 halaman1 s2.0 S2256208714001308 MainMarnia SulfianaBelum ada peringkat
- 1 s2.0 S0022399914000269 MainDokumen5 halaman1 s2.0 S0022399914000269 MainMarnia SulfianaBelum ada peringkat
- Archive of SID: The Effect of Ginger Biscuit On Nausea and Vomiting in Early PregnancyDokumen6 halamanArchive of SID: The Effect of Ginger Biscuit On Nausea and Vomiting in Early PregnancyMarnia SulfianaBelum ada peringkat
- 1 s2.0 S1521690X08001711 MainDokumen18 halaman1 s2.0 S1521690X08001711 MainMarnia SulfianaBelum ada peringkat
- Ginger PDFDokumen14 halamanGinger PDFShinta Maya SariBelum ada peringkat
- 7064 12300 1 PB PDFDokumen11 halaman7064 12300 1 PB PDFMita RestuBelum ada peringkat
- Archive of SID: The Effect of Ginger Biscuit On Nausea and Vomiting in Early PregnancyDokumen6 halamanArchive of SID: The Effect of Ginger Biscuit On Nausea and Vomiting in Early PregnancyMarnia SulfianaBelum ada peringkat
- Mengkudu THDP HTDokumen7 halamanMengkudu THDP HTichalsajaBelum ada peringkat
- 1 s2.0 S1521690X0800170X MainDokumen14 halaman1 s2.0 S1521690X0800170X MainMarnia SulfianaBelum ada peringkat
- 3872 ID Pengaruh Pemberian Jus Buah Belimbing Dan Mentimun Terhadap Penurunan Tekanan Da PDFDokumen10 halaman3872 ID Pengaruh Pemberian Jus Buah Belimbing Dan Mentimun Terhadap Penurunan Tekanan Da PDFdesy irawatiBelum ada peringkat
- Accepted Manuscript: 10.1016/j.nut.2015.01.013Dokumen20 halamanAccepted Manuscript: 10.1016/j.nut.2015.01.013Marnia SulfianaBelum ada peringkat
- Best Practice & Research Clinical Endocrinology & MetabolismDokumen12 halamanBest Practice & Research Clinical Endocrinology & MetabolismMarnia SulfianaBelum ada peringkat
- Asian Nursing Research: Nejla Canbulat, PHD, Sevil - Inal, PHD, Hacer Sönmezer, MSCDokumen6 halamanAsian Nursing Research: Nejla Canbulat, PHD, Sevil - Inal, PHD, Hacer Sönmezer, MSCMarnia SulfianaBelum ada peringkat
- 1 s2.0 S1751722211000928 MainDokumen7 halaman1 s2.0 S1751722211000928 MainMarnia SulfianaBelum ada peringkat
- Antimicrobial Agents: General ConsiderationDokumen19 halamanAntimicrobial Agents: General ConsiderationMarnia SulfianaBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Structures and Functions of the SkinDokumen33 halamanStructures and Functions of the SkinVas LillaBelum ada peringkat
- Sexually Transmitted Diseases: John Potayr E Jude Moscos ODokumen19 halamanSexually Transmitted Diseases: John Potayr E Jude Moscos OJenna OlileBelum ada peringkat
- Waterborne Diseases: Group 2Dokumen21 halamanWaterborne Diseases: Group 2Jay RickBelum ada peringkat
- Postural DrainageDokumen6 halamanPostural DrainageKit Alizon Barredo0% (1)
- My 6-Step Plan For Diagnosing & Managing The Pruritic DogDokumen6 halamanMy 6-Step Plan For Diagnosing & Managing The Pruritic DogAnonymous TDI8qdYBelum ada peringkat
- ScoliosisDokumen4 halamanScoliosisDharline Abbygale Garvida AgullanaBelum ada peringkat
- Morpheus8 Consent FormDokumen3 halamanMorpheus8 Consent FormOnurBelum ada peringkat
- Coma-Causes, Diagnosis, Treatment and ManagementDokumen19 halamanComa-Causes, Diagnosis, Treatment and ManagementHabtamu AdimasuBelum ada peringkat
- CV: Professor of Public HealthDokumen5 halamanCV: Professor of Public HealthDevi SaragihBelum ada peringkat
- Medical Certificate Form For Non Immigrant O A Long Stay OnlyDokumen1 halamanMedical Certificate Form For Non Immigrant O A Long Stay OnlyFiroz KhanBelum ada peringkat
- MCQ 2019 Part 1 UseDokumen94 halamanMCQ 2019 Part 1 UseMimmey YeniwBelum ada peringkat
- FluDokumen31 halamanFluSheril Sularte CasanesBelum ada peringkat
- Coronavirus PCRDokumen1 halamanCoronavirus PCRSyedBelum ada peringkat
- Vital Signs Assessment TableDokumen2 halamanVital Signs Assessment Tableapi-250869701Belum ada peringkat
- Tekilu Isreal 2003Dokumen64 halamanTekilu Isreal 2003Alemayehu KebedeBelum ada peringkat
- Travelers DiarrheaDokumen23 halamanTravelers Diarrheakakang chuBelum ada peringkat
- Neuropsychiatry of Headache PDFDokumen185 halamanNeuropsychiatry of Headache PDFGuillermo GonzalezBelum ada peringkat
- ED Management of Abused ChildDokumen63 halamanED Management of Abused ChildRam Kirubakar ThangarajBelum ada peringkat
- Microbial Diseases of The Nervous SystemDokumen7 halamanMicrobial Diseases of The Nervous SystemAnaBelum ada peringkat
- Safety Health ProtocolsDokumen16 halamanSafety Health ProtocolsTeacher MelBelum ada peringkat
- Case 1 - Pneumonia (Final)Dokumen4 halamanCase 1 - Pneumonia (Final)Joegie ArioBelum ada peringkat
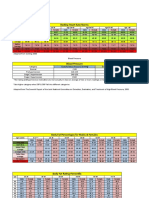
- Resting Heart Rate NormsDokumen3 halamanResting Heart Rate Normstre100% (1)
- The Association of Torch Infection and Congenital Malformations: A Prospective Study in ChinaDokumen36 halamanThe Association of Torch Infection and Congenital Malformations: A Prospective Study in ChinaAisyah MajidBelum ada peringkat
- Tom J Sciatica SlidesDokumen45 halamanTom J Sciatica Slidesgemichan26100% (1)
- Mendelian Randomization Study of Inflammatory Bowel Disease and Bone Mineral DensityDokumen19 halamanMendelian Randomization Study of Inflammatory Bowel Disease and Bone Mineral DensityYaumil ChoiriBelum ada peringkat
- FORUMDokumen4 halamanFORUMGan Jia JingBelum ada peringkat
- SKRINING Dan Penerapannya Pada Proses Skrining ISPA Pasien Balita Di Daerah Banjarbaru PPT English VersionDokumen11 halamanSKRINING Dan Penerapannya Pada Proses Skrining ISPA Pasien Balita Di Daerah Banjarbaru PPT English VersionYulia Afrina NstBelum ada peringkat
- SIRS, qSOFA, and Organ Failure For Assessing Sepsis at The Emergency DepartmentDokumen4 halamanSIRS, qSOFA, and Organ Failure For Assessing Sepsis at The Emergency DepartmentAnnitaCristalBelum ada peringkat
- MAN Para-title-Manuscript - Cathy-TurianoDokumen43 halamanMAN Para-title-Manuscript - Cathy-TurianoSevered AppleheadBelum ada peringkat
- Slow Contact Tracing' Blamed For Spread of New CoronavirusDokumen6 halamanSlow Contact Tracing' Blamed For Spread of New CoronavirusProdigal RanBelum ada peringkat