Anda mungkin juga menyukai
- Cause and Effects of Substance Abuse Among The Students Community480Dokumen15 halamanCause and Effects of Substance Abuse Among The Students Community480Suman MondalBelum ada peringkat
- Mental DisorderDokumen5 halamanMental DisorderHijaz TurohaBelum ada peringkat
- CTS India Medical Insurance Policy 2017 - 18Dokumen34 halamanCTS India Medical Insurance Policy 2017 - 18nivasshaan100% (2)
- HPV Vaccine Gardasil Crosses Blood-Brain Barrier and Causes Cerebral VasculitisDokumen11 halamanHPV Vaccine Gardasil Crosses Blood-Brain Barrier and Causes Cerebral VasculitisMoralVolcano100% (8)
- Gowri .P Gowri .P Gowri .P Gowri .P Gowri .P: "ThokkanamDokumen15 halamanGowri .P Gowri .P Gowri .P Gowri .P Gowri .P: "Thokkanamsesha1234100% (2)
- Questions For Community Medicine MD 4Dokumen11 halamanQuestions For Community Medicine MD 4Bindashboy0Belum ada peringkat
- The Psychology of Pain: George R. Hansen, MD, Jon Streltzer, MDDokumen10 halamanThe Psychology of Pain: George R. Hansen, MD, Jon Streltzer, MDRobi Maulana100% (1)
- Viral Encephalitis PDFDokumen7 halamanViral Encephalitis PDFDeborah Bravian TairasBelum ada peringkat
- Nature - Bipolar DisordersDokumen16 halamanNature - Bipolar DisordersVanessa LealBelum ada peringkat
- HIV and Mental HealthDokumen7 halamanHIV and Mental HealthAyu RajikanBelum ada peringkat
- Grades 7-9 Life Orientation CapsDokumen27 halamanGrades 7-9 Life Orientation CapsngeleBelum ada peringkat
- Hamilton Anxiety Rating Scale (HAM-A)Dokumen2 halamanHamilton Anxiety Rating Scale (HAM-A)Elsa Ameliana ManurungBelum ada peringkat
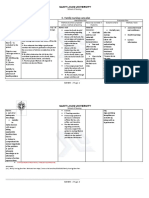
- C. Family Nursing Care Plan: Saint Louis UniversityDokumen2 halamanC. Family Nursing Care Plan: Saint Louis UniversityLEONELLGABRIEL RAGUINDIN0% (1)
- Questions 1-10: Blubber For Protection and They Are Almost Completely HairlessDokumen14 halamanQuestions 1-10: Blubber For Protection and They Are Almost Completely HairlessAisyah75% (4)
- Assignment On Historcal Evolution of Research in NursingDokumen17 halamanAssignment On Historcal Evolution of Research in NursingKavi rajput50% (2)
- Envejecimiento HivDokumen8 halamanEnvejecimiento HivJose LunaBelum ada peringkat
- 2012 delPalacioM HIV1Infection RevMedVirolDokumen14 halaman2012 delPalacioM HIV1Infection RevMedVirolvictorcdBelum ada peringkat
- Hiv EncephalopathyDokumen37 halamanHiv EncephalopathyIndah LatifahBelum ada peringkat
- Smith 2008Dokumen27 halamanSmith 2008Lindia PrabhaswariBelum ada peringkat
- Molecular Mechanisms of Neuroinvasion by Monocytes-Macrophages in HIV-1 InfectionDokumen11 halamanMolecular Mechanisms of Neuroinvasion by Monocytes-Macrophages in HIV-1 InfectionRiddhi GandhiBelum ada peringkat
- Neurologic Presentationsofaids: Elyse J. Singer,, Miguel Valdes-Sueiras,, Deborah Commins,, Andrew LevineDokumen23 halamanNeurologic Presentationsofaids: Elyse J. Singer,, Miguel Valdes-Sueiras,, Deborah Commins,, Andrew LevineBigBoostingBelum ada peringkat
- SNC Sin TBCDokumen23 halamanSNC Sin TBCFernando ArancibiaBelum ada peringkat
- Eng Ver Kalinowska PDFDokumen10 halamanEng Ver Kalinowska PDFReynatta Audralia NamaraBelum ada peringkat
- A Comparison Between HIV-Associated Neurocognitive Disorder (HAND) and Long Covid - A Systematic ReviewDokumen10 halamanA Comparison Between HIV-Associated Neurocognitive Disorder (HAND) and Long Covid - A Systematic ReviewEstefanía Rivas-García (Fefa)Belum ada peringkat
- Aspectos Neuropsiquiatricos VihDokumen35 halamanAspectos Neuropsiquiatricos VihCarolina MuñozBelum ada peringkat
- HIV-1-associated Neurocognitive Disorder - Epidemiology, Pathogenesis, Diagnosis, and TreatmentDokumen13 halamanHIV-1-associated Neurocognitive Disorder - Epidemiology, Pathogenesis, Diagnosis, and Treatmenthasbi.alginaaBelum ada peringkat
- HIV-Associated Neurologic Disorders and Central Nervous System Opportunistic Infections in HIVDokumen9 halamanHIV-Associated Neurologic Disorders and Central Nervous System Opportunistic Infections in HIVYanuar Ahsan OfficialBelum ada peringkat
- Neurological Complications of HIV Infection: Central Nervous System Infections (K Bloch, Section Editor)Dokumen7 halamanNeurological Complications of HIV Infection: Central Nervous System Infections (K Bloch, Section Editor)Sadam Yondaime AriesBelum ada peringkat
- Dementia and Neurocognitive Disorders Due To HIV-1 InfectionDokumen7 halamanDementia and Neurocognitive Disorders Due To HIV-1 Infectionmira ariantiBelum ada peringkat
- Psychiatric Aspects of HIV Invection and AIDSDokumen28 halamanPsychiatric Aspects of HIV Invection and AIDSKiky SymbiontBelum ada peringkat
- CROI 2019 Neurologic Complications of HIV DiseaseDokumen8 halamanCROI 2019 Neurologic Complications of HIV DiseaseErick Paúl Bazán MoyaBelum ada peringkat
- Infectious MyelopathiesDokumen23 halamanInfectious MyelopathiesAnonymous 7jKR9XbBelum ada peringkat
- Infectious Causes of Seizures and Epilepsy in The Developing WorldDokumen11 halamanInfectious Causes of Seizures and Epilepsy in The Developing WorldRebecca WilliamsBelum ada peringkat
- Human Immunodeficiency Virus-Associated Dementia: Review of Pathogenesis, Prophylaxis, and Treatment Studies of Zidovudine TherapyDokumen16 halamanHuman Immunodeficiency Virus-Associated Dementia: Review of Pathogenesis, Prophylaxis, and Treatment Studies of Zidovudine TherapyRiddhi GandhiBelum ada peringkat
- Neuropsychiatric Manifestationsofhiv-1 Infectionandaids: Dwightl - Evans Kareni - Mason Janeleserman Russellbauer JohnpetittoDokumen19 halamanNeuropsychiatric Manifestationsofhiv-1 Infectionandaids: Dwightl - Evans Kareni - Mason Janeleserman Russellbauer JohnpetittoInomy Claudia Katherine ImbiriBelum ada peringkat
- Paediatric Acute Encephalitis: Infection and InflammationDokumen10 halamanPaediatric Acute Encephalitis: Infection and InflammationRajeshKoriyaBelum ada peringkat
- Arbovírus PDFDokumen49 halamanArbovírus PDFSabrina ParenteBelum ada peringkat
- Emailing Neurological Complications of Infectious Diseases, 2021Dokumen389 halamanEmailing Neurological Complications of Infectious Diseases, 2021Zeeshan KarimBelum ada peringkat
- Neuropsychiatric Complications of Hiv/aidsDokumen3 halamanNeuropsychiatric Complications of Hiv/aidsInomy Claudia Katherine ImbiriBelum ada peringkat
- HIV Nephropathy - StatPearls - NCBI BookshelfDokumen5 halamanHIV Nephropathy - StatPearls - NCBI BookshelfEmmanuel SoteloBelum ada peringkat
- Neuroimaging in The Brain in HIV-1-Infected PatientsDokumen25 halamanNeuroimaging in The Brain in HIV-1-Infected PatientsYanina Pérez de VillarrealBelum ada peringkat
- Clinical Aspects of Headache in HIVDokumen8 halamanClinical Aspects of Headache in HIVnatacha479Belum ada peringkat
- Acute Viral Encephalitis - NEJMDokumen17 halamanAcute Viral Encephalitis - NEJMFredghcBelum ada peringkat
- JC Virus 2.0.Dokumen9 halamanJC Virus 2.0.Kartheek VarmaBelum ada peringkat
- Human Immunodeficiency Virus (Hiv) & Sexually Transmitted Infections (Sti)Dokumen37 halamanHuman Immunodeficiency Virus (Hiv) & Sexually Transmitted Infections (Sti)Nicola4Belum ada peringkat
- Headache Among Patient With HIV DeseaseDokumen12 halamanHeadache Among Patient With HIV DeseaseAbdullah QayyumBelum ada peringkat
- Psychiatric Aspects of HIV Spectrum DiseaseDokumen8 halamanPsychiatric Aspects of HIV Spectrum DiseaseInomy Claudia Katherine ImbiriBelum ada peringkat
- Insights Pathogenesis Therapeutic: ProgressiveDokumen11 halamanInsights Pathogenesis Therapeutic: ProgressiveDewi NofiantiBelum ada peringkat
- 02 NewhorizonsDokumen8 halaman02 NewhorizonsgloriaBelum ada peringkat
- Rar Vol11 Nro3Dokumen21 halamanRar Vol11 Nro3Valentine WijayaBelum ada peringkat
- Neurology 08Dokumen6 halamanNeurology 08MohammedSalmanAhmedBelum ada peringkat
- Potentiation of Excitotoxicity in HIV-1-associated Dementia and The Significance of GlutaminaseDokumen14 halamanPotentiation of Excitotoxicity in HIV-1-associated Dementia and The Significance of GlutaminaseRiddhi GandhiBelum ada peringkat
- PAH and HIV Journal Hearth and LungDokumen4 halamanPAH and HIV Journal Hearth and LungFelisa Nur KhayanaBelum ada peringkat
- Viral Encephalitis: A Clinician's Guide: Practical NeurologyDokumen19 halamanViral Encephalitis: A Clinician's Guide: Practical NeurologyCésar Vásquez Aguilar100% (1)
- HIV-Associated Opportunistic Infections of The CNSDokumen13 halamanHIV-Associated Opportunistic Infections of The CNSmauroignacioBelum ada peringkat
- International Journal of Infectious Diseases: A A B A A A A A A A A B ADokumen9 halamanInternational Journal of Infectious Diseases: A A B A A A A A A A A B AzikryauliaBelum ada peringkat
- The Management of Encephalitis Clinical Practice Guidelines by The Infectious Diseases Society of AmericaDokumen25 halamanThe Management of Encephalitis Clinical Practice Guidelines by The Infectious Diseases Society of AmericaNana ShkodinaBelum ada peringkat
- Infecciones Oportunistas Del SNC en VIH LAncet 2010Dokumen13 halamanInfecciones Oportunistas Del SNC en VIH LAncet 2010Natalia Obando LermaBelum ada peringkat
- Epidemiology of EncephalitisDokumen2 halamanEpidemiology of EncephalitisFarhan Royan PermanahadiBelum ada peringkat
- Whitley1991 Article HerpesSimplexVirusInfectionsOfDokumen22 halamanWhitley1991 Article HerpesSimplexVirusInfectionsOfjaspforeverBelum ada peringkat
- Diagnosis and Clinical Features of Major Neuropsychiatric Disorders in HIV InfectionDokumen9 halamanDiagnosis and Clinical Features of Major Neuropsychiatric Disorders in HIV InfectionOscar Alejandro Cardenas QuinteroBelum ada peringkat
- 1 s2.0 S1521690X99900477 MainDokumen19 halaman1 s2.0 S1521690X99900477 MainAzarudeenBelum ada peringkat
- Had 1Dokumen14 halamanHad 1Riddhi GandhiBelum ada peringkat
- Depression and Diagnosis of NeurocognitiveDokumen14 halamanDepression and Diagnosis of Neurocognitivejeams manuBelum ada peringkat
- Balneo 319Dokumen6 halamanBalneo 319Mihaela MavrodinBelum ada peringkat
- Immediate and Long-Term Consequences of COVID-19 Infections For The Development of Neurological DiseaseDokumen3 halamanImmediate and Long-Term Consequences of COVID-19 Infections For The Development of Neurological DiseaseMaca Martínez-CuitiñoBelum ada peringkat
- HHS Public Access: Prevention of Stroke in People Living With HIVDokumen22 halamanHHS Public Access: Prevention of Stroke in People Living With HIVMartha OktaviaBelum ada peringkat
- Chapter 6Dokumen11 halamanChapter 6KurbulBelum ada peringkat
- HIV and PsychiatryDari EverandHIV and PsychiatryJohn A. JoskaBelum ada peringkat
- Clinical Neuroimmunology: Multiple Sclerosis and Related DisordersDari EverandClinical Neuroimmunology: Multiple Sclerosis and Related DisordersBelum ada peringkat
- Lai 2015Dokumen13 halamanLai 2015tugba1234Belum ada peringkat
- Obtaining International Excellence Through Cross-Border Research Initiatives: A Consortium-Sponsored JournalDokumen1 halamanObtaining International Excellence Through Cross-Border Research Initiatives: A Consortium-Sponsored Journaltugba1234Belum ada peringkat
- Accepted Manuscript: Drug and Alcohol DependenceDokumen33 halamanAccepted Manuscript: Drug and Alcohol Dependencetugba1234Belum ada peringkat
- Ijbs 09 216Dokumen5 halamanIjbs 09 216tugba1234Belum ada peringkat
- Mindfulness: Implications For Substance Abuse and AddictionDokumen7 halamanMindfulness: Implications For Substance Abuse and Addictiontugba1234Belum ada peringkat
- The Hypothalamic-pituitary-Adrenal Axis in Anxiety and PanicDokumen6 halamanThe Hypothalamic-pituitary-Adrenal Axis in Anxiety and Paniccitra dewiBelum ada peringkat
- Dual Diagnosis and Quality of Life in Patients in Treatment For Opioid DependenceDokumen12 halamanDual Diagnosis and Quality of Life in Patients in Treatment For Opioid Dependencetugba1234Belum ada peringkat
- Maybe 2 PDFDokumen18 halamanMaybe 2 PDFSheryl ElitaBelum ada peringkat
- Video Stres OksidatifDokumen7 halamanVideo Stres Oksidatiftugba1234Belum ada peringkat
- Phenomenology of SchizophreniaDokumen7 halamanPhenomenology of Schizophreniatugba1234Belum ada peringkat
- Phenomenology of SchizophreniaDokumen7 halamanPhenomenology of Schizophreniatugba1234Belum ada peringkat
- GWL InaDokumen25 halamanGWL Inatugba1234Belum ada peringkat
- Dr. Hendro-Parallel Symposium 8 PDFDokumen15 halamanDr. Hendro-Parallel Symposium 8 PDFtugba1234Belum ada peringkat
- What Is DepressionDokumen5 halamanWhat Is Depressiontugba1234Belum ada peringkat
- Behavioural Weight Loss Intervention With Serious Mentall IllnessDokumen9 halamanBehavioural Weight Loss Intervention With Serious Mentall Illnesstugba1234Belum ada peringkat
- Psikolog Distress PD TBCDokumen9 halamanPsikolog Distress PD TBCtugba1234Belum ada peringkat
- ARRDokumen2 halamanARRtugba1234Belum ada peringkat
- 11 Anti Anxiety DrugsDokumen17 halaman11 Anti Anxiety Drugstugba1234Belum ada peringkat
- Depression Among ODHA JamaicaDokumen5 halamanDepression Among ODHA Jamaicatugba1234Belum ada peringkat
- Classification of Psychiatric Disorders: Ug Class Dept. of PsychiatryDokumen26 halamanClassification of Psychiatric Disorders: Ug Class Dept. of Psychiatrytugba1234Belum ada peringkat
- Tech Titan Usb Anti-Virus User Manual The Ultimate USB Anti-Virus Featured in This Product Is Powered by Kaspersky LabDokumen24 halamanTech Titan Usb Anti-Virus User Manual The Ultimate USB Anti-Virus Featured in This Product Is Powered by Kaspersky Labtugba1234Belum ada peringkat
- Prognosis Apprisal Sheet PDFDokumen2 halamanPrognosis Apprisal Sheet PDFAkhmad AfriantoBelum ada peringkat
- Geriatric Psychiatry, 14: 858-865.: Daftar PustakaDokumen5 halamanGeriatric Psychiatry, 14: 858-865.: Daftar Pustakatugba1234Belum ada peringkat
- Psikotropika Obat Acuan PenggolonganDokumen6 halamanPsikotropika Obat Acuan Penggolongantugba1234Belum ada peringkat
- Prevalence of Depression in People Living With HIV/AIDS Undergoing ART and Factors Associated With ItDokumen9 halamanPrevalence of Depression in People Living With HIV/AIDS Undergoing ART and Factors Associated With Ittugba1234Belum ada peringkat
- NIH Public Access: Suicidal Thoughts and Behavior With Antidepressant TreatmentDokumen15 halamanNIH Public Access: Suicidal Thoughts and Behavior With Antidepressant Treatmenttugba1234Belum ada peringkat
- Simpson Angus ScaleDokumen6 halamanSimpson Angus ScaleManish KumarBelum ada peringkat
- Amnesia and Crime: Dominique Bourget, MD, and Laurie Whitehurst, PHDDokumen12 halamanAmnesia and Crime: Dominique Bourget, MD, and Laurie Whitehurst, PHDtugba1234Belum ada peringkat
- Treatment and PerceptionsDokumen24 halamanTreatment and Perceptionstugba1234Belum ada peringkat
- Cba Syllabus - Fin SC Tech Most RecentDokumen70 halamanCba Syllabus - Fin SC Tech Most RecentEpie FranklineBelum ada peringkat
- Abnormal Psychology Overview Research ApproachesDokumen52 halamanAbnormal Psychology Overview Research ApproachesBatshidi SelebogoBelum ada peringkat
- Conf Program FINAL31212Dokumen156 halamanConf Program FINAL31212Anand gowdaBelum ada peringkat
- Kankanaey Cultures 1Dokumen10 halamanKankanaey Cultures 1hanzellebganBelum ada peringkat
- Impaired Tissue PerfusionDokumen2 halamanImpaired Tissue PerfusionLeo Mar MakilanBelum ada peringkat
- MPH-Model Course CurriculumDokumen24 halamanMPH-Model Course CurriculumRyan WootenBelum ada peringkat
- Journal of Developing Drugs: Self-Medication Trends in Children by Their ParentsDokumen7 halamanJournal of Developing Drugs: Self-Medication Trends in Children by Their ParentsNisa Puspita TrisnasaryBelum ada peringkat
- World Psychiatry June 2017Dokumen112 halamanWorld Psychiatry June 2017Marco Macavilca CruzBelum ada peringkat
- LAS For Summative Assessment (Written Work Performance Task)Dokumen2 halamanLAS For Summative Assessment (Written Work Performance Task)Angel Dela CruzBelum ada peringkat
- Infectious Laryngotracheitis in Poultry: Razol RazalanDokumen27 halamanInfectious Laryngotracheitis in Poultry: Razol RazalanLemuel Lagasca Razalan IVBelum ada peringkat
- FTR Registration FormDokumen2 halamanFTR Registration Formpinipini367% (6)
- Abdellah's 21 Nursing Problem TheoryDokumen14 halamanAbdellah's 21 Nursing Problem TheoryJyoti Verma100% (1)
- Mapeh Reviewer 3rd QuarterDokumen3 halamanMapeh Reviewer 3rd QuarterIceyYamaha60% (5)
- Unit 11 Introduction To EpidemiologyDokumen38 halamanUnit 11 Introduction To EpidemiologyhumaBelum ada peringkat
- Imei Cardiac DiseaseDokumen4 halamanImei Cardiac DiseaseMakBelum ada peringkat
- A.Haleem (2020) Areas of Academic Research With The Impact of COVID-19Dokumen8 halamanA.Haleem (2020) Areas of Academic Research With The Impact of COVID-19Azizan RamlyBelum ada peringkat
- HED205Dokumen98 halamanHED205Kingsley AmakaBelum ada peringkat
- Chapter 1 To The End New FinalDokumen54 halamanChapter 1 To The End New FinalClarence PalmaBelum ada peringkat
- Prova de Proficiência em Leitura - Inglês - UFPA - Modelo 1Dokumen3 halamanProva de Proficiência em Leitura - Inglês - UFPA - Modelo 1DANIELLEBelum ada peringkat