Anda mungkin juga menyukai
- Seminar On Upper Limb FractureDokumen166 halamanSeminar On Upper Limb FractureArko dutta100% (1)
- Fractures: Pathophysiology and EtiologyDokumen5 halamanFractures: Pathophysiology and EtiologyHafid JuniorBelum ada peringkat
- Orthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Dokumen13 halamanOrthopaedic Surgery Fractures and Dislocations: Tomas Kurakovas MF LL Group 29Tomas Kurakovas100% (1)
- FracturesDokumen26 halamanFracturesMelinda MelinBelum ada peringkat
- EVALUATE AND TREAT ORTHOPEDIC INJURIESDokumen24 halamanEVALUATE AND TREAT ORTHOPEDIC INJURIESvikramBelum ada peringkat
- Trauma - Intertrochanteric Fracture - RustiniDokumen7 halamanTrauma - Intertrochanteric Fracture - Rustinidedyalkarni08Belum ada peringkat
- Classification of FracturesDokumen26 halamanClassification of FracturesHoney May Rollan VicenteBelum ada peringkat
- Lo MSK 2-3Dokumen6 halamanLo MSK 2-3FirmanHidayatBelum ada peringkat
- Orthopaedic EssaysDokumen139 halamanOrthopaedic EssaysDuncan Jackson100% (1)
- Orthopedic InjuriesDokumen27 halamanOrthopedic InjuriesvikramBelum ada peringkat
- تروما محاضرة 1Dokumen58 halamanتروما محاضرة 1202003339Belum ada peringkat
- Principles of Bone FracturesDokumen59 halamanPrinciples of Bone Fracturesanwar jabariBelum ada peringkat
- Fractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaDokumen50 halamanFractures: Mary Grace B. Gutierrez Resti Mariano Ma. Cindy O. BautistaJustin Ahorro-DionisioBelum ada peringkat
- Dr. Chowdhury Iqbal Mahmud: MBBS, Frcs (Uk), MCH (Ortho, Uk)Dokumen48 halamanDr. Chowdhury Iqbal Mahmud: MBBS, Frcs (Uk), MCH (Ortho, Uk)Chowdhury Iqbal MahmudBelum ada peringkat
- General Principles of Fractures: Department of Orthopaedic Surgery Liu Xueyong (刘学勇)Dokumen82 halamanGeneral Principles of Fractures: Department of Orthopaedic Surgery Liu Xueyong (刘学勇)Banna Kiran KumarBelum ada peringkat
- MusculoskelealDokumen32 halamanMusculoskelealEbuka AniBelum ada peringkat
- Fracture Nursing Care Management: Study GuideDokumen5 halamanFracture Nursing Care Management: Study Guidezahwa ayundaBelum ada peringkat
- Introduction of FractureDokumen80 halamanIntroduction of Fracturealsead798Belum ada peringkat
- Common Orthopedic Emergency Conditions and Their ManagementDokumen6 halamanCommon Orthopedic Emergency Conditions and Their ManagementDhruva PatelBelum ada peringkat
- FRACTUREDokumen16 halamanFRACTUREPriyaBelum ada peringkat
- Types and Treatment of FracturesDokumen68 halamanTypes and Treatment of FracturesokaciaBelum ada peringkat
- Traumatic InjuryDokumen64 halamanTraumatic InjuryDYRAH GRACE COPAUSBelum ada peringkat
- Fractures: Types, Complications, and ManagementDokumen26 halamanFractures: Types, Complications, and Managementsm - kardmBelum ada peringkat
- Fracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaDokumen96 halamanFracture: Suchithra.P.V 1 Year Msc. Nursing College of Nursing AlappuzhaAakash A. AgrawalBelum ada peringkat
- Fracture Types and ManagementDokumen53 halamanFracture Types and Managementrahul yadav100% (7)
- Tibial Plateau and Shaft Fractures GuideDokumen22 halamanTibial Plateau and Shaft Fractures GuidevadimmadanBelum ada peringkat
- Schwartz Ortho NotesDokumen16 halamanSchwartz Ortho Notesfsf50% (2)
- Fractures GuidelinesDokumen73 halamanFractures GuidelinesChester Abraham LongaBelum ada peringkat
- Principles of Fractures: (Continued)Dokumen44 halamanPrinciples of Fractures: (Continued)Abdi Ñãśìr Møhàmèď ŚàĺàhBelum ada peringkat
- Fracture 01Dokumen42 halamanFracture 01api-19916399Belum ada peringkat
- Ortho - Surgery PDFDokumen15 halamanOrtho - Surgery PDFIC BBelum ada peringkat
- Introduction To Fracture, Bone Healing and Complication: Prof - DR Jameel - Tahseen Mehsen Trauma and Orthopedics SurgeonDokumen20 halamanIntroduction To Fracture, Bone Healing and Complication: Prof - DR Jameel - Tahseen Mehsen Trauma and Orthopedics Surgeonحسين رسول ناجيBelum ada peringkat
- Skeletal Trauma-Plain Film Trauma Terminology ReviewDokumen35 halamanSkeletal Trauma-Plain Film Trauma Terminology Reviewbjpalmer100% (3)
- Types of Fractures and Healing StagesDokumen45 halamanTypes of Fractures and Healing Stagesanupama varghese100% (1)
- NCP: Nursing Care Plan For Bone FracturesDokumen8 halamanNCP: Nursing Care Plan For Bone FracturesElham TabaoBelum ada peringkat
- Management of Musculoskeletal InjuriesDokumen102 halamanManagement of Musculoskeletal InjuriesMaria Lynne Parambita100% (1)
- Fractures and Low Back Pain: Dr. Lubna DwerijDokumen49 halamanFractures and Low Back Pain: Dr. Lubna DwerijNoor MajaliBelum ada peringkat
- Fractures Diagnosis and TreatmentDokumen5 halamanFractures Diagnosis and TreatmentubaycentralBelum ada peringkat
- Percutaneous Osteosynthesis of The Distal Fractures of The Femur. Eladio Saura Mendoza e Eladio Saura SanchezDokumen12 halamanPercutaneous Osteosynthesis of The Distal Fractures of The Femur. Eladio Saura Mendoza e Eladio Saura SanchezNuno Craveiro LopesBelum ada peringkat
- ORIF Radius and Ulna ProcedureDokumen7 halamanORIF Radius and Ulna ProcedurealcojonicBelum ada peringkat
- Orthopedic: Dislocations of The Hip JointDokumen16 halamanOrthopedic: Dislocations of The Hip JointAnmarBelum ada peringkat
- FrakturDokumen188 halamanFrakturSiti RaihanatiBelum ada peringkat
- Fracturesgoutosteosprain 2Dokumen199 halamanFracturesgoutosteosprain 2Rose Cristille Yeso JocsonBelum ada peringkat
- Musculoskeletal Disorders FRACTURESDokumen10 halamanMusculoskeletal Disorders FRACTURESرافت العواضيBelum ada peringkat
- Pembahasan TTG FrakturDokumen48 halamanPembahasan TTG FrakturErik Ad'perdianBelum ada peringkat
- Orthopedic EmergenciesDokumen75 halamanOrthopedic EmergenciesAlex beharuBelum ada peringkat
- Understanding Intertrochanteric Fractures of the FemurDokumen12 halamanUnderstanding Intertrochanteric Fractures of the FemurEinz Nur Amalyah IdrusBelum ada peringkat
- Musculoskeletal Fractures GuideDokumen8 halamanMusculoskeletal Fractures GuideandreeaBelum ada peringkat
- 1 Classifications of FracturesDokumen33 halaman1 Classifications of Fracturesرغد شاكر محمود أحمدBelum ada peringkat
- General Principles of FractureDokumen31 halamanGeneral Principles of Fractureamel015Belum ada peringkat
- Comprehensive SummaryDokumen37 halamanComprehensive Summaryhrg79qzwc2Belum ada peringkat
- Types of Bone Fractures and Common Traction MethodsDokumen3 halamanTypes of Bone Fractures and Common Traction MethodsMarc AnchetaBelum ada peringkat
- Orthopedic NursingDokumen23 halamanOrthopedic Nursinggabrielle magdaraog100% (1)
- Orthopedic: Clinical Features of FracturesDokumen6 halamanOrthopedic: Clinical Features of FracturesDrAyyoub AbboodBelum ada peringkat
- Knee and Leg Injuries: Causes, Symptoms, TreatmentsDokumen14 halamanKnee and Leg Injuries: Causes, Symptoms, TreatmentsDrAyyoub AbboodBelum ada peringkat
- FIX - Fracture and DislocationDokumen80 halamanFIX - Fracture and DislocationWildan Hilmi AnsoriBelum ada peringkat
- Orthopedics Condensed MaterialDokumen13 halamanOrthopedics Condensed Materialhznknzbwk7Belum ada peringkat
- Comprehensive Guide to the General Approach and Management of Orthopedic Trauma and FracturesDokumen14 halamanComprehensive Guide to the General Approach and Management of Orthopedic Trauma and FracturesJeffrey Ariesta PutraBelum ada peringkat
- Distal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsDari EverandDistal Clavicle Osteolysis, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsBelum ada peringkat
- MSF - Financial - Report - 2021 - FINAL ProvisionalDokumen78 halamanMSF - Financial - Report - 2021 - FINAL ProvisionaldcgfdcBelum ada peringkat
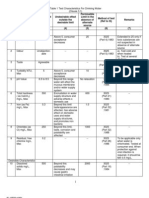
- Drinking Water - Is 10500-1991 PDFDokumen3 halamanDrinking Water - Is 10500-1991 PDFearthanskyfriends100% (1)
- Legal and Policy Mechanisms for Urban Pollution ControlDokumen511 halamanLegal and Policy Mechanisms for Urban Pollution ControlPASTOR STARBelum ada peringkat
- Supervisory Relationship GuideDokumen4 halamanSupervisory Relationship GuideremamadhavaBelum ada peringkat
- Mobility - Nursing Test QuestionsDokumen91 halamanMobility - Nursing Test QuestionsRNStudent1100% (3)
- Financial Behavior of Millenial Genration On Investment DecisionDokumen8 halamanFinancial Behavior of Millenial Genration On Investment DecisionYuslia Nandha Anasta SariBelum ada peringkat
- Cancer FungusDokumen2 halamanCancer FungusRajesh KumarBelum ada peringkat
- Cyanotic Congenital Heart Disease With Decreased Pulmonary Blood FlowDokumen7 halamanCyanotic Congenital Heart Disease With Decreased Pulmonary Blood FlowdrhomiedanBelum ada peringkat
- IMer C Research CompetitionDokumen1 halamanIMer C Research CompetitiongabbynengBelum ada peringkat
- Hayrax Con Mascara Facial PDFDokumen8 halamanHayrax Con Mascara Facial PDFSantos LopBelum ada peringkat
- Law Oblicon :) )Dokumen9 halamanLaw Oblicon :) )Fiona MoralesBelum ada peringkat
- HSE L123 - 2016 - Health Care and First Aid On Offshore Installions and Pipeline WorksDokumen31 halamanHSE L123 - 2016 - Health Care and First Aid On Offshore Installions and Pipeline WorksKris WilochBelum ada peringkat
- The Centaur: Magazine From Centaur Services LimitedDokumen28 halamanThe Centaur: Magazine From Centaur Services LimitedStela SilvaBelum ada peringkat
- Trauma Copiilor AbandonatiDokumen132 halamanTrauma Copiilor AbandonatiPaula CelsieBelum ada peringkat
- King's Speech Speech Impediment OvercomeDokumen3 halamanKing's Speech Speech Impediment OvercomeMichael KesslerBelum ada peringkat
- IAEA SSR-3 - Safety of Research ReactorsDokumen152 halamanIAEA SSR-3 - Safety of Research Reactorsmadalina_troneaBelum ada peringkat
- Constructing Temporary Access Road for Geothermal PlantDokumen3 halamanConstructing Temporary Access Road for Geothermal PlantGad100% (6)
- Confined Space Rescue PlanDokumen10 halamanConfined Space Rescue PlanNick Shelley100% (2)
- Alternative Work Arrangement November 16-20, 2020Dokumen4 halamanAlternative Work Arrangement November 16-20, 2020Maria Kristel L PascualBelum ada peringkat
- Toronto Public Health Absenteeism Notification LetterDokumen2 halamanToronto Public Health Absenteeism Notification LetterToronto StarBelum ada peringkat
- NCP of MGH PatientDokumen2 halamanNCP of MGH PatientMaverick LimBelum ada peringkat
- Book Review: Mastery of Hand Strength (1st Edition) : Wednesday, February 11, 2009Dokumen8 halamanBook Review: Mastery of Hand Strength (1st Edition) : Wednesday, February 11, 2009Ernesto MoraBelum ada peringkat
- Aesthetic Management of Immediate Anterior Tooth Replacement With Ovate Pontic: A Case Report PDFDokumen5 halamanAesthetic Management of Immediate Anterior Tooth Replacement With Ovate Pontic: A Case Report PDFAnita PrastiwiBelum ada peringkat
- Level 2 Certificate in Understanding Behaviour That ChallengesDokumen26 halamanLevel 2 Certificate in Understanding Behaviour That Challenges0115Nurul Haque EmonBelum ada peringkat
- Adolescence: An Age of Storm and Stress: Saba HashmiDokumen15 halamanAdolescence: An Age of Storm and Stress: Saba HashmiVANDANA MISHRABelum ada peringkat
- Dent 336: Endodontics Course SyllabusDokumen9 halamanDent 336: Endodontics Course SyllabusFiru LgsBelum ada peringkat
- Ingredients:: The Lemonade Diet (Adapted From)Dokumen2 halamanIngredients:: The Lemonade Diet (Adapted From)test100% (2)
- Project Report On Herbal Extraction UnitDokumen17 halamanProject Report On Herbal Extraction UnitEIRI Board of Consultants and PublishersBelum ada peringkat
- Good Will HuntingDokumen2 halamanGood Will HuntingkyshbBelum ada peringkat
- Austin Kraft ResumeDokumen2 halamanAustin Kraft Resumeapi-384086145Belum ada peringkat