Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Normative Symbol Digit Modalities Test..Dokumen7 halamanNormative Symbol Digit Modalities Test..baobhBelum ada peringkat
- Tales of The Sinful StarsDokumen199 halamanTales of The Sinful Starsshorn100% (3)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Basic Engineering Correlation Calculus v3 001Dokumen3 halamanBasic Engineering Correlation Calculus v3 001Ska doosh100% (1)
- F-500 Encapsulator TechnologyDokumen6 halamanF-500 Encapsulator TechnologyBdSulianoBelum ada peringkat
- Text Linguistics and Classical Studies - Facebook Com LinguaLIBDokumen129 halamanText Linguistics and Classical Studies - Facebook Com LinguaLIBEnglish Buzz100% (1)
- Introduction To PragmaticsDokumen119 halamanIntroduction To PragmaticsIsabella IsaBella75% (4)
- SOP's For All Digital Marketing ActivitesDokumen3 halamanSOP's For All Digital Marketing ActivitesSavijeet Singh50% (2)
- 12 F 08 TMTDokumen2 halaman12 F 08 TMTbaobhBelum ada peringkat
- Tratamiento Farmacologico TLPDokumen9 halamanTratamiento Farmacologico TLPbaobhBelum ada peringkat
- Sex Related Neuro Anatomical Basis of Emotion RegulationDokumen7 halamanSex Related Neuro Anatomical Basis of Emotion RegulationbaobhBelum ada peringkat
- HPA Madres Lactantes y EmbarazadasDokumen13 halamanHPA Madres Lactantes y EmbarazadasbaobhBelum ada peringkat
- X Linked Genes Mental FunctioningDokumen6 halamanX Linked Genes Mental FunctioningbaobhBelum ada peringkat
- Serum BDNF LevelsDokumen6 halamanSerum BDNF LevelsbaobhBelum ada peringkat
- Genetic Regulation BDNFDokumen14 halamanGenetic Regulation BDNFbaobhBelum ada peringkat
- CashDokumen6 halamanCashbaobh0% (1)
- Diferencias Sexuales en El Estrés CrónicoDokumen20 halamanDiferencias Sexuales en El Estrés CrónicobaobhBelum ada peringkat
- Andy - Riley. .Return - Of.bunny - SuicidesDokumen90 halamanAndy - Riley. .Return - Of.bunny - SuicidesJohn Popet Garcia100% (1)
- CNT SVX15D E4 1111Dokumen60 halamanCNT SVX15D E4 1111Mihai IavorschiBelum ada peringkat
- Coreldraw 12 Hotkeys - Keyboard ShortcutsDokumen6 halamanCoreldraw 12 Hotkeys - Keyboard ShortcutsRais AhmadBelum ada peringkat
- Design of Bulk CarrierDokumen7 halamanDesign of Bulk CarrierhoangductuanBelum ada peringkat
- Player PrefsDokumen1 halamanPlayer PrefsHafiz AbdulwahabBelum ada peringkat
- Lab 2 ECADokumen7 halamanLab 2 ECAAizan AhmedBelum ada peringkat
- 2 (Molecular Diffusion in Gases)Dokumen66 halaman2 (Molecular Diffusion in Gases)Nasir ShamsBelum ada peringkat
- Active FilterDokumen16 halamanActive FilterRam SankarBelum ada peringkat
- Refining of MaterialsDokumen38 halamanRefining of MaterialsJAWAD AHMAD BURTBelum ada peringkat
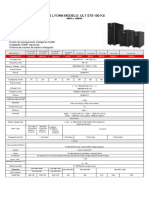
- Ups Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVADokumen1 halamanUps Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVASebastian Matias CruzBelum ada peringkat
- Surge Current Protection Using SuperconductorDokumen25 halamanSurge Current Protection Using SuperconductorAbhishek Walter PaulBelum ada peringkat
- CE 205 - Analyzing Hydrographs and Deriving Unit HydrographsDokumen17 halamanCE 205 - Analyzing Hydrographs and Deriving Unit HydrographsUmange RanasingheBelum ada peringkat
- Types of Nuclear Reactors GuideDokumen19 halamanTypes of Nuclear Reactors GuideUgur GuvenBelum ada peringkat
- Word Processing and Desktop Publishing SoftwareDokumen24 halamanWord Processing and Desktop Publishing SoftwareMubarak KashiBelum ada peringkat
- Experimental Noize Guitar Set 1 Effects PedalDokumen2 halamanExperimental Noize Guitar Set 1 Effects PedalSingani Titicaca100% (1)
- 2 Nuts and Bolts: 2.1 Deterministic vs. Randomized AlgorithmsDokumen13 halaman2 Nuts and Bolts: 2.1 Deterministic vs. Randomized AlgorithmsEdmund ZinBelum ada peringkat
- Manual X-C EFC Diversey Namthip - ENDokumen37 halamanManual X-C EFC Diversey Namthip - ENthouche007Belum ada peringkat
- One Plus 7Dokumen114 halamanOne Plus 7Priyanka ChudasamaBelum ada peringkat
- Mathematical Induction, Peano Axioms, and Properties of Addition of Non-Negative IntegersDokumen13 halamanMathematical Induction, Peano Axioms, and Properties of Addition of Non-Negative IntegersMarius PaunescuBelum ada peringkat
- RMI Verif NAFEMS 3 2 PDFDokumen28 halamanRMI Verif NAFEMS 3 2 PDFFernando MartinezBelum ada peringkat
- IO SystemDokumen32 halamanIO Systemnanekaraditya06Belum ada peringkat
- MediaanditsterilzationDokumen15 halamanMediaanditsterilzationAyushi MauryaBelum ada peringkat
- KTG Week 1Dokumen22 halamanKTG Week 1Rebecca Soriano SantosBelum ada peringkat
- Structural Geology From Barmer Basin (India)Dokumen12 halamanStructural Geology From Barmer Basin (India)Sankhajit SahaBelum ada peringkat
- Fiber Optics Unit 3Dokumen82 halamanFiber Optics Unit 3NIKHIL SOLOMON P URK19CS1045Belum ada peringkat
- Holiday Assignment XDokumen2 halamanHoliday Assignment XMonis ShaikhBelum ada peringkat