Anda mungkin juga menyukai
- Analysis of Blood Lactate and Heart Rate of Indoor SportsDokumen4 halamanAnalysis of Blood Lactate and Heart Rate of Indoor SportsAlmiraNadiaBelum ada peringkat
- A Method-Comparison Study Regarding - LactateDokumen7 halamanA Method-Comparison Study Regarding - LactateAlmiraNadiaBelum ada peringkat
- Training Intensity DistributionDokumen17 halamanTraining Intensity DistributiondashhamidmamaliBelum ada peringkat
- Athlete Handbook AntidopingDokumen40 halamanAthlete Handbook AntidopingAlmiraNadiaBelum ada peringkat
- Blood TestDokumen4 halamanBlood TestMustafa Al ZawawiBelum ada peringkat
- SalerioDokumen28 halamanSalerioRizqaFebrilianyBelum ada peringkat
- Armstrong LE Review Paper Assessing HydrationDokumen10 halamanArmstrong LE Review Paper Assessing HydrationAlmiraNadiaBelum ada peringkat
- Lirik MoccaDokumen25 halamanLirik MoccaAlmiraNadiaBelum ada peringkat
- Faktor Determinan Risiko Osteoporosis Di Tiga Provinsi Di IndonesiaDokumen9 halamanFaktor Determinan Risiko Osteoporosis Di Tiga Provinsi Di IndonesiaSenja TsamrotulBelum ada peringkat
- Sea Cucumber FarmingDokumen6 halamanSea Cucumber Farmingmorisrav23Belum ada peringkat
- VLN VC Mendelssohn Wedding March PartsDokumen2 halamanVLN VC Mendelssohn Wedding March PartsAlmiraNadiaBelum ada peringkat
- Am J Clin Nutr-2005-Abrams-471-6 Prebiotics Short ChainDokumen6 halamanAm J Clin Nutr-2005-Abrams-471-6 Prebiotics Short ChainAlmiraNadiaBelum ada peringkat
- Faktor Determinan Risiko Osteoporosis Di Tiga Provinsi Di IndonesiaDokumen9 halamanFaktor Determinan Risiko Osteoporosis Di Tiga Provinsi Di IndonesiaSenja TsamrotulBelum ada peringkat
- Prebiotics, Probiotics, and Synbiotics AffectDokumen9 halamanPrebiotics, Probiotics, and Synbiotics AffectAlmiraNadiaBelum ada peringkat
- 117 631 1 PB PDFDokumen12 halaman117 631 1 PB PDFAlmiraNadiaBelum ada peringkat
- Diet, Nutrition and Bone Health - InulinDokumen6 halamanDiet, Nutrition and Bone Health - InulinAlmiraNadiaBelum ada peringkat
- Collagen-Hydroxyapatite Composites For Hard Tissue RepairDokumen14 halamanCollagen-Hydroxyapatite Composites For Hard Tissue RepairAlmiraNadiaBelum ada peringkat
- Prebiotics, Probiotics, and Synbiotics AffectDokumen9 halamanPrebiotics, Probiotics, and Synbiotics AffectAlmiraNadiaBelum ada peringkat
- 117 631 1 PB PDFDokumen12 halaman117 631 1 PB PDFAlmiraNadiaBelum ada peringkat
- Collagen TreatmentDokumen8 halamanCollagen TreatmentAlmiraNadiaBelum ada peringkat
- Collagen ExtarctionDokumen5 halamanCollagen ExtarctionAlmiraNadiaBelum ada peringkat
- Koolman, 368 Bettelheim, 507-508 Ensiklopedia of Pshycal Science and Technology, 338,201-220Dokumen1 halamanKoolman, 368 Bettelheim, 507-508 Ensiklopedia of Pshycal Science and Technology, 338,201-220AlmiraNadiaBelum ada peringkat
- Millon Nasse TestDokumen12 halamanMillon Nasse TestAlmiraNadiaBelum ada peringkat
- P ('t':'3', 'I':'670993317') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)Dokumen7 halamanP ('t':'3', 'I':'670993317') D '' Var B Location Settimeout (Function ( If (Typeof Window - Iframe 'Undefined') ( B.href B.href ) ), 15000)AlmiraNadiaBelum ada peringkat
- 3385-4137-1-SM Formula F 100 Who PDFDokumen14 halaman3385-4137-1-SM Formula F 100 Who PDFAlmiraNadiaBelum ada peringkat
- Tamia Dwi Anindita: The Relationship of Body Image Perception and EatingDokumen1 halamanTamia Dwi Anindita: The Relationship of Body Image Perception and EatingAlmiraNadiaBelum ada peringkat
- Nutrisi Dan Gizi BurukDokumen9 halamanNutrisi Dan Gizi BurukFifin HestiBelum ada peringkat
- Eoryeodo Apeun Geon Ttok Gata-2AMDokumen4 halamanEoryeodo Apeun Geon Ttok Gata-2AMIndriani SavitriBelum ada peringkat
- Pengaruh Lama Dan Suhu Pengeringan Terhadap Mutu Tepung PandanDokumen74 halamanPengaruh Lama Dan Suhu Pengeringan Terhadap Mutu Tepung PandanAlmiraNadiaBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Principles and Practice of Chiropractic, 3E (2005) (PDF) (UnitedVRG)Dokumen1.246 halamanPrinciples and Practice of Chiropractic, 3E (2005) (PDF) (UnitedVRG)Maikell Moura79% (14)
- Europass Curriculum Vitae: Personal Information Popescu Simona-AlinaDokumen11 halamanEuropass Curriculum Vitae: Personal Information Popescu Simona-AlinaTanveerBelum ada peringkat
- The Prevention and Management of Congenital SyphilDokumen10 halamanThe Prevention and Management of Congenital Syphillink_wolfloboBelum ada peringkat
- Removable Orthodontic ApplianceDokumen7 halamanRemovable Orthodontic ApplianceAhmed AymanBelum ada peringkat
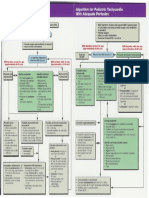
- Pediatric Tachycardia AlgorithmsDokumen1 halamanPediatric Tachycardia AlgorithmsGalih FatoniBelum ada peringkat
- Directive or Non-Directive Genetic Counselling - Cutting Through The SurfaceDokumen6 halamanDirective or Non-Directive Genetic Counselling - Cutting Through The Surfacejsus22Belum ada peringkat
- LIFE Kite Flying Sponsorship LetterDokumen3 halamanLIFE Kite Flying Sponsorship LetterMarjorie CuaBelum ada peringkat
- Bone MuscleDokumen433 halamanBone Muscleridho budiBelum ada peringkat
- Strabismus 10Dokumen25 halamanStrabismus 10william williamBelum ada peringkat
- Medicolegal ProblemsDokumen2 halamanMedicolegal ProblemsBabith Moses WilbyBelum ada peringkat
- Physician Resource DirectoryDokumen56 halamanPhysician Resource DirectoryMedStarNRHBelum ada peringkat
- Bisphenol A Epoxy ResinDokumen1 halamanBisphenol A Epoxy ResincnhathoangBelum ada peringkat
- Hypertensive Crisis: Megat Mohd Azman Bin AdzmiDokumen34 halamanHypertensive Crisis: Megat Mohd Azman Bin AdzmiMegat Mohd Azman AdzmiBelum ada peringkat
- PONV Prophylaxis Guidelines: Risk Factor OR 95% CIDokumen4 halamanPONV Prophylaxis Guidelines: Risk Factor OR 95% CIHerly NurrahmaBelum ada peringkat
- James Brazelle Res OtaDokumen4 halamanJames Brazelle Res Otaapi-300158819Belum ada peringkat
- MAPEH (Health) : Quarter 1 - Module 7: Consumer Health: Enrichment For Modules 1-3Dokumen11 halamanMAPEH (Health) : Quarter 1 - Module 7: Consumer Health: Enrichment For Modules 1-3Albert Ian CasugaBelum ada peringkat
- Complete Denture Occlusion PDFDokumen25 halamanComplete Denture Occlusion PDFÄpriolia SuBelum ada peringkat
- A To Z Orthodontics MCQDokumen112 halamanA To Z Orthodontics MCQUjjwal Pyakurel100% (4)
- Licensing Requirement For Acute-Chronic Psychiatric Facility - DOHDokumen3 halamanLicensing Requirement For Acute-Chronic Psychiatric Facility - DOHAgnes Cheverloo CastilloBelum ada peringkat
- A Night at The Museum: Roll Up ! Roll Up! Museums IncDokumen1 halamanA Night at The Museum: Roll Up ! Roll Up! Museums IncKeeranmayeeishraBelum ada peringkat
- FINAL Use and Application of Topical FluoridesDokumen7 halamanFINAL Use and Application of Topical FluoridesmahmoudBelum ada peringkat
- Drug Therapy During Pregnancy and Breast-FeedingDokumen52 halamanDrug Therapy During Pregnancy and Breast-FeedingSonam SonamBelum ada peringkat
- Data Individu 1033017Dokumen14 halamanData Individu 1033017Setyowati DwiBelum ada peringkat
- Feu83 The Stars Are BackDokumen142 halamanFeu83 The Stars Are Backralphdaniel100% (3)
- 2nd Announcement The 4th Scientific Meeting Updates in Neurology 2018 FinalDokumen38 halaman2nd Announcement The 4th Scientific Meeting Updates in Neurology 2018 FinalayuBelum ada peringkat
- Oklahoma State Medical Association Observership Program ApplicationDokumen3 halamanOklahoma State Medical Association Observership Program Applicationredhotdevil1987Belum ada peringkat
- Lapsus Fraktur Neck FemurDokumen32 halamanLapsus Fraktur Neck FemurZóélkårnåín PhåntómhívéBelum ada peringkat
- Blowing The WhistleDokumen4 halamanBlowing The WhistleJeffrey Ventre MD DC100% (2)
- Prevalence and Clinical Features of Cutaneous Leishmaniasis in Dembidolo District, Western Ethiopia: A Cross-Sectional StudyDokumen8 halamanPrevalence and Clinical Features of Cutaneous Leishmaniasis in Dembidolo District, Western Ethiopia: A Cross-Sectional StudyyeniBelum ada peringkat
- William TDokumen7 halamanWilliam Ttony_chrisBelum ada peringkat