Anda mungkin juga menyukai
- Final Na!!! Patho Ko Stab WoundDokumen1 halamanFinal Na!!! Patho Ko Stab WoundWesley BlasBelum ada peringkat
- Buerger's Disease PathophysiologyDokumen3 halamanBuerger's Disease PathophysiologyBon Guevarra SagunBelum ada peringkat
- Careplan Sexual Dysfuntion DyspareuniaDokumen12 halamanCareplan Sexual Dysfuntion DyspareuniaAxus War0% (1)
- Lung Cancer (Nursing Care)Dokumen5 halamanLung Cancer (Nursing Care)heiyuBelum ada peringkat
- Diagram of Pathophysiology CancerDokumen5 halamanDiagram of Pathophysiology CancerKristaMaeC.Lazo0% (3)
- Impaired Skin IntegrityDokumen4 halamanImpaired Skin IntegrityMarjorie Jofel Cerrudo PaciaBelum ada peringkat
- Final Lung Cancer Concept MapDokumen3 halamanFinal Lung Cancer Concept MapKaycee TolingBelum ada peringkat
- Pathophysiology PTBDokumen1 halamanPathophysiology PTBNikki Galvez Braganza100% (2)
- PP - Community-Acquired PneumoniaDokumen1 halamanPP - Community-Acquired Pneumonialpetallo100% (2)
- Patho Pleural EffusionDokumen2 halamanPatho Pleural EffusionJess Prodigo50% (2)
- Pathophysiology - AppendicitisDokumen5 halamanPathophysiology - AppendicitisAzielle Joyce RosquetaBelum ada peringkat
- Dengue Fever Discharge PlanDokumen9 halamanDengue Fever Discharge PlanTrisha Faye OrtegaBelum ada peringkat
- NCP Impaired Gas Exhange CHEST INJURYDokumen4 halamanNCP Impaired Gas Exhange CHEST INJURYMa. Elaine Carla Tating100% (2)
- DRUG STUDY: Bactidol - HexetidineDokumen2 halamanDRUG STUDY: Bactidol - HexetidineYum CBelum ada peringkat
- Thrombophlebitis PathophysiologyDokumen2 halamanThrombophlebitis PathophysiologyKartika YuliantiBelum ada peringkat
- Drug Study FDokumen3 halamanDrug Study FFatima Love Ariate-ArcasetasBelum ada peringkat
- Predisposing Factors Age Diet Dehydration Precipitating Factors Family or Personal History Digestive Diseases and SurgeryDokumen2 halamanPredisposing Factors Age Diet Dehydration Precipitating Factors Family or Personal History Digestive Diseases and SurgeryChloé Jane HilarioBelum ada peringkat
- SchistosomiasisDokumen92 halamanSchistosomiasisIvan Juan75% (4)
- Nursing Care Plan On Foul-Smelling LochiaDokumen3 halamanNursing Care Plan On Foul-Smelling LochiaNE Tdr100% (1)
- DaflonDokumen1 halamanDaflonx483xD50% (2)
- Drug Study in PneumoniaDokumen17 halamanDrug Study in PneumoniaKara Kathrina FuentesBelum ada peringkat
- TAHBSO PathophysiologyDokumen5 halamanTAHBSO Pathophysiologybregette50% (2)
- Macronutrients-Carbohydrates: NCM 105A Nutrition and Diet Therapy Laborator YDokumen3 halamanMacronutrients-Carbohydrates: NCM 105A Nutrition and Diet Therapy Laborator YArriane Desepeda100% (1)
- Pathophysiology of AppendicitisDokumen3 halamanPathophysiology of AppendicitisArvin Ian Penaflor100% (3)
- Pathophysiology of Gastric AdenocarcinomaDokumen2 halamanPathophysiology of Gastric AdenocarcinomaAjon Veloso100% (3)
- Case Chronic Renal Failure Discharge PlanningDokumen2 halamanCase Chronic Renal Failure Discharge PlanningFatima Dorcas Roxas LabausaBelum ada peringkat
- Pathophysiology of Bronchial AsthmaDokumen2 halamanPathophysiology of Bronchial AsthmaFirenze Fil100% (21)
- NCP - Risk For InfectionDokumen2 halamanNCP - Risk For InfectionJet Bautista100% (1)
- Case Management and InnovativeDokumen2 halamanCase Management and InnovativeNur SanaaniBelum ada peringkat
- Tramadol (Dolcet)Dokumen1 halamanTramadol (Dolcet)Beverly Ann de LeonBelum ada peringkat
- Copd PathDokumen2 halamanCopd Pathnursing concept maps100% (2)
- Drug Study CefuroximeDokumen2 halamanDrug Study CefuroximeDave Michael GeliBelum ada peringkat
- Abdominal Stab Wound Case StudyDokumen36 halamanAbdominal Stab Wound Case StudyMean Elepaño80% (5)
- Cancer Nursing Care Plan (NCP) - Risk For InfectionDokumen2 halamanCancer Nursing Care Plan (NCP) - Risk For InfectionAngie MandeoyaBelum ada peringkat
- Bronchial Asthma PathophysiologyDokumen1 halamanBronchial Asthma PathophysiologyElisa Kerr100% (2)
- Betty Knight's "6F S": FluidsDokumen1 halamanBetty Knight's "6F S": FluidsESTHER OGODOBelum ada peringkat
- Pa Tho Physiology of Hiatal HerniaDokumen1 halamanPa Tho Physiology of Hiatal HerniaChiskie Faldas Genodia100% (1)
- 1st Week Reflection - EditedDokumen2 halaman1st Week Reflection - EditedAmrit Acharya100% (1)
- Concept Map HypovolemiaDokumen3 halamanConcept Map HypovolemiaAllyssa Mackinnon67% (3)
- NCP Ineffective Airway Clearance Related To Presence of Secretion in Trachea-Bronchial Tree Secondary To History of CAPDokumen2 halamanNCP Ineffective Airway Clearance Related To Presence of Secretion in Trachea-Bronchial Tree Secondary To History of CAPpa3kmedina100% (1)
- CellulitisDokumen39 halamanCellulitisMary Jhane Villanueva50% (4)
- Pathophysiology Acute GastritisDokumen4 halamanPathophysiology Acute GastritisKaloy Kamao100% (2)
- Drug StudyDokumen14 halamanDrug StudyJenniferValmocenaBelum ada peringkat
- Doxofylline: D 400 MG TabletsDokumen33 halamanDoxofylline: D 400 MG TabletsBibek Singh Mahat100% (2)
- Gordon's Bisaya VersionDokumen2 halamanGordon's Bisaya VersionDanielle Valerie100% (1)
- Calvit Tablet/Suspension: Generic Name: Category: CompositionDokumen2 halamanCalvit Tablet/Suspension: Generic Name: Category: CompositiondentsavvyBelum ada peringkat
- Absence of Responsible Member and Financial ConstraintsDokumen2 halamanAbsence of Responsible Member and Financial ConstraintsFavor ColaBelum ada peringkat
- Pathophysiology of Alzheimers DiseaseDokumen2 halamanPathophysiology of Alzheimers DiseaseJaysellePuguonTabijeBelum ada peringkat
- NCP Ch31 p991-992Dokumen2 halamanNCP Ch31 p991-992Ala'a Abd Mansor100% (2)
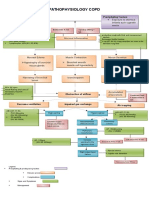
- Pathophysiology of Chronic Obstructive Pulmonary DisorderDokumen2 halamanPathophysiology of Chronic Obstructive Pulmonary DisorderBlessyl Mae EstenzoBelum ada peringkat
- Drugs SevofluraneDokumen9 halamanDrugs Sevofluranequincym75% (4)
- Iv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing FactorsDokumen2 halamanIv. Pathophysiology 1. Schematic Diagram Book Based Pathophysiology: Precipitating/Modifiable Factors Non Modifiable / Predisposing Factorsikemas67% (6)
- Family Nursing Care Plan - Cough and ColdsDokumen1 halamanFamily Nursing Care Plan - Cough and ColdsArnx QuilonBelum ada peringkat
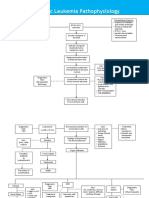
- Acute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsDokumen3 halamanAcute Lymphoblastic Leukemia Pathophysiology: Predisposing Factors: Etiology: Precipitating FactorsKyla ValenciaBelum ada peringkat
- Thoracic TraumaDokumen63 halamanThoracic Traumaheny seri meritaBelum ada peringkat
- Case Study For Pleural-EffusionDokumen10 halamanCase Study For Pleural-EffusionGabbii CincoBelum ada peringkat
- Pleural Diseases WordDokumen7 halamanPleural Diseases WordAbid RasheedBelum ada peringkat
- Tension MedscapeDokumen24 halamanTension MedscapeHandayaniBelum ada peringkat
- Pneumothorax: by Amera GumamaDokumen20 halamanPneumothorax: by Amera GumamaGumama AmeiyrhaBelum ada peringkat
- Pleural Conditions: Pleurisy (Pleuritis)Dokumen10 halamanPleural Conditions: Pleurisy (Pleuritis)merin sunilBelum ada peringkat
- Classification Mechanism of Action Indications Contraindication S Side Effects Nursing Responsibilities Generic Name: PrecautionDokumen1 halamanClassification Mechanism of Action Indications Contraindication S Side Effects Nursing Responsibilities Generic Name: PrecautionJaessa FelicianoBelum ada peringkat
- IsoketDokumen2 halamanIsoketJaessa Feliciano100% (1)
- IsoketDokumen2 halamanIsoketJaessa FelicianoBelum ada peringkat
- People Vs Peralta, Et AlDokumen11 halamanPeople Vs Peralta, Et AlJaessa FelicianoBelum ada peringkat
- Just Another Sebaceous Cyst?: I. Clinical QuestionDokumen3 halamanJust Another Sebaceous Cyst?: I. Clinical QuestionJaessa FelicianoBelum ada peringkat
- DobutamineDokumen2 halamanDobutamineJaessa FelicianoBelum ada peringkat
- DigoxinDokumen4 halamanDigoxinJaessa FelicianoBelum ada peringkat
- Sequioa Hotel: Prepared byDokumen13 halamanSequioa Hotel: Prepared byJaessa Feliciano100% (1)
- Baylon RatioDokumen4 halamanBaylon RatioJaessa Feliciano100% (1)
- Different Types of Stones in Cholelithiasis: Gala John Michael ADokumen2 halamanDifferent Types of Stones in Cholelithiasis: Gala John Michael AJaessa FelicianoBelum ada peringkat
- ER Drug StudyDokumen13 halamanER Drug StudyJaessa FelicianoBelum ada peringkat
- Drug Study and NCP TemplateDokumen3 halamanDrug Study and NCP TemplateJaessa FelicianoBelum ada peringkat
- Vi. Laboratory Results Hematology Result Test Name S.I. Result Unit Reference Range Interpretation & Analysis Hemoglobin Hematocrit White Blood CountDokumen2 halamanVi. Laboratory Results Hematology Result Test Name S.I. Result Unit Reference Range Interpretation & Analysis Hemoglobin Hematocrit White Blood CountJaessa FelicianoBelum ada peringkat
- 3 IdiotsDokumen7 halaman3 IdiotsJaessa FelicianoBelum ada peringkat
- Body Part Normal Findings Actual Findings Data Gaps/ Inconsistencies SkinDokumen9 halamanBody Part Normal Findings Actual Findings Data Gaps/ Inconsistencies SkinJaessa FelicianoBelum ada peringkat
- Minsan Pagising Gising Ako Sa Gabi Kasi Ang Init, Sobra. Kahit Na May Electric Fan.Dokumen2 halamanMinsan Pagising Gising Ako Sa Gabi Kasi Ang Init, Sobra. Kahit Na May Electric Fan.Jaessa FelicianoBelum ada peringkat
- 51 100Dokumen18 halaman51 100Jaessa Feliciano100% (1)
- Name of Drug FinalDokumen7 halamanName of Drug FinalJaessa FelicianoBelum ada peringkat
- Septicemia NCPDokumen3 halamanSepticemia NCPJaessa Feliciano0% (1)
- ChenezDokumen2 halamanChenezJaessa FelicianoBelum ada peringkat
- Estimated Cancer Incidence and Mortality (2012)Dokumen2 halamanEstimated Cancer Incidence and Mortality (2012)Jaessa FelicianoBelum ada peringkat
- Health and Welfare Committee ReportDokumen4 halamanHealth and Welfare Committee ReporttncircuitriderBelum ada peringkat
- Survey QuestionnaireDokumen2 halamanSurvey Questionnairecyrusbatayan100% (1)
- Risk Assessment - GardenDokumen2 halamanRisk Assessment - GardenOlivia BrookesBelum ada peringkat
- About The Author-James Herriot: A Triumph of Surgery Chapter - 1 Footprint Without FeetDokumen4 halamanAbout The Author-James Herriot: A Triumph of Surgery Chapter - 1 Footprint Without FeetSunil rathi100% (3)
- Labor and Delivery OB Concept MapDokumen2 halamanLabor and Delivery OB Concept MapMissy Johnson75% (4)
- Mental HealthDokumen14 halamanMental Healthapi-455779994100% (1)
- English Teacher's NotesDokumen24 halamanEnglish Teacher's NotesPrincess KimBelum ada peringkat
- YakultDokumen15 halamanYakultMlb T. De TorresBelum ada peringkat
- BURNS SoftDokumen3 halamanBURNS SoftErlo John Asentista0% (1)
- Lab 11 AntianginalDokumen4 halamanLab 11 AntianginalanaBelum ada peringkat
- PHC Assignment 1Dokumen5 halamanPHC Assignment 1Florenze Laiza Donor Lucas100% (1)
- Community-Based Disaster Risk Reduction and Management Training CourseDokumen3 halamanCommunity-Based Disaster Risk Reduction and Management Training CourseMARJORYL CLAISE GONZALESBelum ada peringkat
- Presentation of Neurogenic Shock Within The Emergency Department - TaylorDokumen6 halamanPresentation of Neurogenic Shock Within The Emergency Department - TaylorAnprtma kaunangBelum ada peringkat
- VE4 Sem 1 Student Packet (25 July)Dokumen187 halamanVE4 Sem 1 Student Packet (25 July)Dwayne June GetiganBelum ada peringkat
- HeartDokumen12 halamanHeartRebar photographyBelum ada peringkat
- Answers To Questions: Earl John E. CañoneroDokumen2 halamanAnswers To Questions: Earl John E. CañoneroEarl CañoneroBelum ada peringkat
- Consent ModelDokumen4 halamanConsent ModelSundaresan ChockalingamBelum ada peringkat
- CircCircuit Protection in Health Care Facilitiesuit Protection in Health Care FacilitiesDokumen43 halamanCircCircuit Protection in Health Care Facilitiesuit Protection in Health Care FacilitiesMenaBelum ada peringkat
- HKS CannabisDokumen21 halamanHKS CannabisRavioli Boo GaddamBelum ada peringkat
- Meditation ScriptDokumen9 halamanMeditation Scriptapi-361293242100% (1)
- Annual Premium Statement: Bhupesh GuptaDokumen1 halamanAnnual Premium Statement: Bhupesh GuptaBhupesh GuptaBelum ada peringkat
- Potsdam Village Police Dept. Blotter Sept. 10, 2017Dokumen2 halamanPotsdam Village Police Dept. Blotter Sept. 10, 2017NewzjunkyBelum ada peringkat
- 3 5 18 950 PDFDokumen3 halaman3 5 18 950 PDFBang AthanBelum ada peringkat
- Sustainable Rural Water, Sanitation and Hygiene Project PROPOSALDokumen13 halamanSustainable Rural Water, Sanitation and Hygiene Project PROPOSALLawrence WatssonBelum ada peringkat
- Craniofacial SyndromesDokumen101 halamanCraniofacial SyndromesSaranya MohanBelum ada peringkat
- Union Civil Protection Mechanism: More Effective, Efficient and Coherent Disaster ManagementDokumen23 halamanUnion Civil Protection Mechanism: More Effective, Efficient and Coherent Disaster ManagementCătălin Marian IvanBelum ada peringkat
- FDA AuditDokumen3 halamanFDA AuditRazor1011Belum ada peringkat
- Vape Waste Report PAE C3Dokumen14 halamanVape Waste Report PAE C3LVNewsdotcomBelum ada peringkat
- Crane Workbox 4398Dokumen4 halamanCrane Workbox 4398hazopman100% (1)
- MarriottDokumen4 halamanMarriottSheikh Farhan AliBelum ada peringkat