Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Nursing School Necessities Cheat SheetDokumen3 halamanNursing School Necessities Cheat SheetRevBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- 4066-To Perform Hot Work Activities (Welding, Oxy Cutting, Grinding, Cutting, Heat Gun andDokumen3 halaman4066-To Perform Hot Work Activities (Welding, Oxy Cutting, Grinding, Cutting, Heat Gun andEric TingBelum ada peringkat
- School District of Philadelphia's Immigrant & Refugee ToolkitDokumen58 halamanSchool District of Philadelphia's Immigrant & Refugee ToolkitKristina KoppeserBelum ada peringkat
- MediterraneanDokumen39 halamanMediterraneanJeff Lester PiodosBelum ada peringkat
- School Threat AssessmentDokumen12 halamanSchool Threat AssessmentChelsea ElizabethBelum ada peringkat
- The Holy Grail of Curing DPDRDokumen12 halamanThe Holy Grail of Curing DPDRDany Mojica100% (1)
- English Job Solution by Recent PublicationDokumen370 halamanEnglish Job Solution by Recent PublicationHimel100% (1)
- Basic Principles of Cross-Examination: Claire F. RushDokumen14 halamanBasic Principles of Cross-Examination: Claire F. RushSellappan RathinamBelum ada peringkat
- IPAMS Healthcare and Medical Services Evaluation FormDokumen2 halamanIPAMS Healthcare and Medical Services Evaluation FormManases VelasquezBelum ada peringkat
- Sampling Techniques: Advantages and DisadvantagesDokumen1 halamanSampling Techniques: Advantages and DisadvantagesMohamed SamirBelum ada peringkat
- Sampling Techniques: Advantages and DisadvantagesDokumen1 halamanSampling Techniques: Advantages and DisadvantagesMohamed SamirBelum ada peringkat
- Healthcare Evaluation Old Version PDFDokumen217 halamanHealthcare Evaluation Old Version PDFMohamed SamirBelum ada peringkat
- 2013, Translational Medicine-The Future of TherapyDokumen8 halaman2013, Translational Medicine-The Future of TherapyMohamed SamirBelum ada peringkat
- Multiplex Genome Editing To Generate Universal CAR T CellsDokumen33 halamanMultiplex Genome Editing To Generate Universal CAR T CellsMohamed SamirBelum ada peringkat
- Drug ManufacturingDokumen3 halamanDrug ManufacturingMohamed SamirBelum ada peringkat
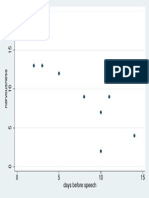
- RegressionDokumen1 halamanRegressionMohamed SamirBelum ada peringkat
- Epidermal Stem CellDokumen9 halamanEpidermal Stem CellMohamed SamirBelum ada peringkat
- Pragmatic Randomized TrialDokumen10 halamanPragmatic Randomized TrialMohamed SamirBelum ada peringkat
- New RegulationDokumen76 halamanNew RegulationMohamed SamirBelum ada peringkat
- Missing Data 2Dokumen1 halamanMissing Data 2Mohamed SamirBelum ada peringkat
- Introduction To PharmacoVigilanceDokumen8 halamanIntroduction To PharmacoVigilanceMohamed SamirBelum ada peringkat
- Pharmaceutical Drug Regulatory AffairsDokumen2 halamanPharmaceutical Drug Regulatory AffairsMohamed SamirBelum ada peringkat
- Pharmaceutical Drug Regulatory AffairsDokumen2 halamanPharmaceutical Drug Regulatory AffairsMohamed SamirBelum ada peringkat
- PediatricDokumen3 halamanPediatricMohamed SamirBelum ada peringkat
- PediatricDokumen3 halamanPediatricMohamed SamirBelum ada peringkat
- Zorn - Stata 4 Dummies - 2007Dokumen12 halamanZorn - Stata 4 Dummies - 2007BooksboyBelum ada peringkat
- Introduction To PharmacoVigilanceDokumen8 halamanIntroduction To PharmacoVigilanceMohamed SamirBelum ada peringkat
- Introduction To Stata 11 Getting Started With Stata Programming by Nicholas P. NicolettiDokumen56 halamanIntroduction To Stata 11 Getting Started With Stata Programming by Nicholas P. NicolettiMohamed Samir100% (1)
- Sop Cleaning Rev 06 - 2018 Rev Baru (Repaired)Dokumen20 halamanSop Cleaning Rev 06 - 2018 Rev Baru (Repaired)FajarRachmadiBelum ada peringkat
- MadRiverUnion01 13 21editionDokumen8 halamanMadRiverUnion01 13 21editionMad River UnionBelum ada peringkat
- Vector and Pest Control in DisastersDokumen10 halamanVector and Pest Control in DisastersTaufik RizkiandiBelum ada peringkat
- English in Nursing 1: Novi Noverawati, M.PDDokumen11 halamanEnglish in Nursing 1: Novi Noverawati, M.PDTiara MahardikaBelum ada peringkat
- Mini BalanzaDokumen146 halamanMini Balanzaisaac_elvisBelum ada peringkat
- Csa Fodrea 2014 - 2015 Student Handbook FinalDokumen37 halamanCsa Fodrea 2014 - 2015 Student Handbook Finalapi-260407035Belum ada peringkat
- Antiparkinsonian Drugs Pathophysiology and TreatmentDokumen5 halamanAntiparkinsonian Drugs Pathophysiology and Treatmentkv 14Belum ada peringkat
- Debona 2016Dokumen23 halamanDebona 2016Biomontec Biomontec BiomontecBelum ada peringkat
- DRRM Plan2020 2021Dokumen5 halamanDRRM Plan2020 2021SheChanBelum ada peringkat
- 15.1 - PH II - Leave Rules-2019Dokumen40 halaman15.1 - PH II - Leave Rules-2019Ranjeet SinghBelum ada peringkat
- Atls 1Dokumen5 halamanAtls 1Mega MalyndaBelum ada peringkat
- UntitledDokumen221 halamanUntitledlaljadeff12Belum ada peringkat
- ManeuversDokumen16 halamanManeuversCezar-George BadaleBelum ada peringkat
- Ekstrak Kulit Buah Naga Super Merah Sebagai Anti-Kanker PayudaraDokumen5 halamanEkstrak Kulit Buah Naga Super Merah Sebagai Anti-Kanker PayudaraWildatul Latifah IIBelum ada peringkat
- Mumps Guide: Causes, Symptoms, Treatment & PreventionDokumen14 halamanMumps Guide: Causes, Symptoms, Treatment & PreventionChristian JonathanBelum ada peringkat
- Written Assignment Unit 7Dokumen7 halamanWritten Assignment Unit 7Edgar PampulahBelum ada peringkat
- Theoretical Models of Nursing Practice AssignmentDokumen6 halamanTheoretical Models of Nursing Practice Assignmentmunabibenard2Belum ada peringkat
- AFP Hemoptysis - 2022Dokumen9 halamanAFP Hemoptysis - 2022Joshua DiaoBelum ada peringkat
- Functional Electrical StimulationDokumen11 halamanFunctional Electrical StimulationMohd Khairul Ikhwan AhmadBelum ada peringkat
- Test Bank For Fundamental Nursing Skills and Concepts Tenth EditionDokumen36 halamanTest Bank For Fundamental Nursing Skills and Concepts Tenth Editionooezoapunitory.xkgyo4100% (41)
- OGL 481 Pro-Seminar I: PCA-Ethical Communities Worksheet Erica KovarikDokumen4 halamanOGL 481 Pro-Seminar I: PCA-Ethical Communities Worksheet Erica Kovarikapi-529016443Belum ada peringkat