IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 9 Ver. VIII (Sep. 2015), PP 51-54
www.iosrjournals.org
Hematological profile of sickle cell disorder in tertiary care
hospital
Dr.Jitendra Chavda1, Dr.Parth Goswami2, Dr.Alpesh Goswami3
1
Assistant Professor, Departement of pathology, Government medical college, Bhavnagar, Gujrat, India
2
Tutor, Departement of pathology, Government medical college, Bhavnagar, Gujrat, India
3
Associate Professor, Departement of pathology, Government medical college, Bhavnagar, Gujrat, India
Abstract:
Introduction: Sickle hemoglobin is the most common pathological hemoglobin mutation worldwide in which
upon deoxygenation RBCs convert into sickle form. Heterozygotes(AS) are usually asymptomatic and
Homozygotes(SS)suffer from sickle cell anemia. Aim: To study hematological profiles of sickle cell disorders
from Sir.T.Hospital, Bhavnagar. Materials and Methods: Prospective cross-sectional study was done in the
Department of pathology, Government medical college, Bhavnagar from January 2013 to May 2015. Blood
collected in EDTA vaccute and hematological indices measured by Abott cell dyne 3700 along with peripheral
smear examination and confirmed by sickle solubility test and Hb electrophoresis. Results: Among 30 cases of
sickle cell disease and 15 cases of sickle cell trait, male most commonly affected with mean age group 10 year.
Hematological profile shows low Hb, MCH, MCHC and Hematocrit values with high MCV. Peripheral smear
demonstrate anisopoikilocytosis(98%),sickle cell(68%) and target cell.(48%). Because sickle cell disorder is
most common hemoglobinopathy such type of study is required which will support for correct diagnosis and
epidemiological analysis.
Key words: sickle cell disease, hematological profiles , peripheral smear.
I.
Introduction
Hb S(Sickle hemoglobin) is abnormal hemoglobin variant in which adenine in sixth codon of beta gene
is substituted by thiamine.So, valine replace glutamic acid in sixth position of beta chain. On deoxygenation of
red blood cells, Hb S form tactoid aggregates and distorts RBCs into sickle shape. Upon oxygenation, these
RBCs regain their normal shape. On repeated sickling and desickling, RBCs convert into permanent sickle
shape. Because of sickle red blood cell anemia, crisis and organ damage can occur.1
Hb S is most common mutation worldwide. Heterozygotes(AS) are usually asymptomatic and
Homozygotes(SS)suffer from sickle cell anemia. Heterozygous carrier patients usually resistant against
malaria.2 50% of world population affected by sickle cell disease resides in India. The average frequency of
sickle cell disease gene ranges between 22-44%.High prevalence is in tribal community of Gujrat, India.3
Hematological profiles of sickle cell disease is extremely variable. There is very little data available on
hematological profiles of sickle cell disease from India. Few studies were undertaken for hemat profile of sickle
cell disease from surat,south gujrat,valsad.4
This study was conducted to study hematological profiles and burden of sickle hemoglobin among
patient visiting at Sir.T.Hospital,Bhavnagar. This will helpful in better diagnosis of sickle cell disease and for
epidemiological study.
II.
Materials And Methods
Prospective cross-sectional study was done in the Department of pathology, Government medical
college, Bhavnagar from January 2013 to may 2015. Data regarding hemoglobin, MCV(mean corpuscular
volume),MCHC(mean corpuscular hemoglobin concentration),MCH(mean corpuscular hemoglobin), RBCs
count, Hematocrit, peripheral blood smear examination ,sickling test and hemoglobin electrophoresis were
noted. Blood collected in ethylene di-aminetetraacetic acid(EDTA) vaccutte and hematological indices were
measured using ABOTT CELL DYN 3700 and peripheral smear stained with leishman stain. Sickling test done
using Sickle solubility test( SICK VIEW) method. To differentiate between disease and trait electrophoresis
done using cellulose acetate strip at alkaline Ph.
III.
Results
In our study total 45 cases were diagnosed as sickle cell disorder. Among them males were more
commonly affected then female with male:female ratio 2:1. Mean age group was 10 year. 30 cases were of
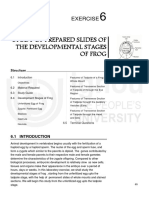
sickle cell disease showing Hb S band and remaining 15 cases showing Hb A and Hb S band that were
diagnosed as sickle cell trait(By cellulose acetate electrophoresis). All cases were positive for SICK VIEW.
DOI: 10.9790/0853-14985154
www.iosrjournals.org
51 | Page
Hematological profile of sickle cell disorder in tertiary care hospital
Figure No. 1
Electrophoresis showing sickle cell trait
Table No. 1 Hematological profiles in sickle cell disorder
Serial no.
1
2
3
4
5
6
Parameters
Hemoglobin value
RBCs count
Hematocrit
MCV
MCH
MCHC
Mean value
8.6 gm/dl
2.8 million/cumm
25%
101 fl
24 pg
26 gm/dl
Table No. 2 Peripheral smear examination in sickle cell disorders
Serial no.
1
2
3
4
5
Parameters
Anisocytosis
Poikilocytosis
Target cells
Sickle cells
Polychromasia
Total no. of case showing particular changes
44(97.77%)
45(100%)
22(48.88%)
31(68.88%)
27(60%)
Diagram No. 1
Peripheral smear changes in sickle cell disorders
120.00%
100.00%
80.00%
60.00%
40.00%
20.00%
Average no.of case
showing particular
changes(In
percentage)
0.00%
Bar diagram illustrate peripheral smear changes in sickle cell disorder
DOI: 10.9790/0853-14985154
www.iosrjournals.org
52 | Page
Hematological profile of sickle cell disorder in tertiary care hospital
Figure No. 3
Peripheral smear showing sickled RBCs,Normoblast and target cells.
IV.
Discussion
In our study males were more as compared to female, which may be due to male child get more
attention as compared to female. Male : female ratio 2:1.Similar result seen in some other study also. 5,6Mean age
group was 10 year which correlates with other study by Shrikhade AV et al.7 in which maximum number of
male patient seen up to age 14 year.
Mean Hb value 8.6 gm/dl that is nearby to other study`s average Hb value which is 7.11 gm/dl. 7 Total
no. of case showing sickle RBCs were 31 while sick view test was positive in all cases. Five cases studied by
shukla RN et al. observed presence of sickle cells and positive for sickling test in all 5 cases. 8 Total RBCs count,
MCH, MCHC are low in our study which is comparable to other study. 9,10MCV is higher than normal, reason
may be because of increased need of erythropoiesis due to chronic hemolysis leading to macrocytosis. 11,12All
sick view positive cases were confirmed as sickle cell disorder by cellulose acetate agar electrophoresis at
alkaline ph. In our study 30 cases(66.66%) were diagnosed as sickle disease and 15 cases(33.33%) were sickle
cell trait by electrophoresis. Study done by Kamble M et all observed 61.6% cases of Hb SS and 38.4% cases of
Hb AS.5
V.
Conclusion
This study shows that MCH, MCHC, RBCs count, hematocrit, hemoglobin value low in sickle cell
disease patients. These patient`s peripheral smear shows anisopoikilocytosis, target cells, sickle RBCs. Further
study can be done using HPLC(High performance liquid chromatography) for quantification of Hb S, if
facilities available for HPLC.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
Winfred C.Wang, Sickle Cell Anemia and other Sickling Syndromes in Wintrobes Clinical Hematology, John P. Greer, John
forester, George M. Rodgers, Frixos Paraskevas, Bertil Glader, Daniel A. Arber, Robert T. Means, Vol 1, eds 12th, Wolters
Kluwer/Lippincott Williams and wilkins, Philedelphia, 2009.pp1038-40.
Piel FB, Patil AP, Hawas RE et al. Global epidemiology of sickle haemoglobin in neonates: contemporary geostatistical model
based map and population estimates. Lancet 2013;38:142-51
B Vasava, R Chudasama, N Godara, R Srivastava. Prevalence of sickle cell disease in tribal adolescents of the South Gujarat region,
India. The Internet Journal of Tropical Medicine. 2008 Volume 6 Number 1.
National
Rural
Health
Mission
Program
Implementation
Plan
201112.
Available
from:
http://pipnrhmmohfw.nic.in/index_files/non_high_focus_large/gujarat/05.%20Chapter%204/4.D%20DCP/10.pdf.
Kamble M, Chaturvedi P. Epidemiology of sickle cell disease in a rural hospital of central India, Indian Pediatr 2000;37:391-6.
Rao S, Goyal JP, Raghunath SV, Shah VB. Hematlogy profile of sickle cell disease from South Gujarat, India. Hematol Rep
2012;4: e8.
Shrikhande AV, Dani AA, Tijare JR, Agrawal AK. Hematological profile of sickle cell disease in central India. Indian J Hematol
Blood Transfus 2007;23:92-8.
Shukla RN, Solanki BR, Parande AS. Sickle cell disease in India.Blood 1958 ;13:552-8.
Roy B, Dey B, Balgir RS, et al. Identification of sickle cell homozygotes using haematological parameters. J Indian Anthrop
Soc. 1996;31:1919.
Tshilolo L, Wembonyama S, Summa V, Avvisati G. [Hemogram findings in Congolese children with sickle cell disease in
remission] Med Trop (Mars)2010;70:45963.
DOI: 10.9790/0853-14985154
www.iosrjournals.org
53 | Page
Hematological profile of sickle cell disorder in tertiary care hospital
[11].
[12].
Figueiredo MS, Kerbauy J, Goncalves MS, et al. Effect of -thalassemia and -globingene cluster haplotypes on the hematological
and clinical features of sickle cell anemia in Brazil. Am J Haematol. 1996;53:727.
Falusi AG, OLatunji PO. Effects of alpha thalassemia and haemoglobin F (HbF) level on the clinical severity of sickle cell
anaemia. Eur J Haematol. 1994;752:135.
DOI: 10.9790/0853-14985154
www.iosrjournals.org
54 | Page
Anda mungkin juga menyukai
- Don Tolman - FDR3 - WholeFoodMedicines PDFDokumen176 halamanDon Tolman - FDR3 - WholeFoodMedicines PDFLerere Allala100% (4)
- Biol 1010 Exam 2 ReviewDokumen3 halamanBiol 1010 Exam 2 Reviewapi-302931792Belum ada peringkat
- Lieshmeniasis IJPSIDokumen3 halamanLieshmeniasis IJPSIdvenumohanBelum ada peringkat
- A Review Literature On Sickle Cell Anemia: Akanksha PatelDokumen21 halamanA Review Literature On Sickle Cell Anemia: Akanksha PatelNoe Essono KolloBelum ada peringkat
- Thalassemia IndiaDokumen4 halamanThalassemia IndiaDr Laxmikant Basavraj DamaBelum ada peringkat
- Nej MoDokumen9 halamanNej MoNadia Mrz Mattew MuseBelum ada peringkat
- Puspa ProjectDokumen39 halamanPuspa Projectshubhamnaik772Belum ada peringkat
- Spectrum of Thalassemia Syndromes and Abnormal Haemoglobins in Adult PatientDokumen4 halamanSpectrum of Thalassemia Syndromes and Abnormal Haemoglobins in Adult PatientBharat MahajanBelum ada peringkat
- DR - Muddassir Final Synopsis..Dokumen22 halamanDR - Muddassir Final Synopsis..Sikander GirgoukarBelum ada peringkat
- NavtejDokumen6 halamanNavtejNavtej kumarBelum ada peringkat
- Study of Spectrum of Hemoglobinopathies in Adult Age Group Diagnosed On High Performance Liquid Chromatography in Tertiary Care HospitalDokumen9 halamanStudy of Spectrum of Hemoglobinopathies in Adult Age Group Diagnosed On High Performance Liquid Chromatography in Tertiary Care HospitalIJAR JOURNALBelum ada peringkat
- Paediatrica Indonesiana: Original ArticleDokumen4 halamanPaediatrica Indonesiana: Original ArticleInge Dackrisna DaudBelum ada peringkat
- 100015IJBTIWI2015 WoldieDokumen5 halaman100015IJBTIWI2015 WoldieSigrid MiBelum ada peringkat
- Sickle Cell Anaemia Literature ReviewDokumen5 halamanSickle Cell Anaemia Literature Reviewc5nc3whz100% (1)
- Literature Review On Sickle Cell AnaemiaDokumen5 halamanLiterature Review On Sickle Cell Anaemiaaflspbnyu100% (1)
- 2.Applied-Elevated Serum Acid Phosphatase-Mamta YadavDokumen4 halaman2.Applied-Elevated Serum Acid Phosphatase-Mamta YadavImpact JournalsBelum ada peringkat
- Shivan ReseachDokumen140 halamanShivan ReseachshjahsjanshaBelum ada peringkat
- BLOOD BANK Storage Related Haematological and Biochemical Changes in Plasmodium Falciparum Infected and Sicle Cell Trait Donor BloodDokumen10 halamanBLOOD BANK Storage Related Haematological and Biochemical Changes in Plasmodium Falciparum Infected and Sicle Cell Trait Donor BloodVincent ReyesBelum ada peringkat
- An Etiological Reappraisal of Pancytopenia - LargestDokumen9 halamanAn Etiological Reappraisal of Pancytopenia - LargestKaye Antonette AntioquiaBelum ada peringkat
- RBC Histogram As Diagnostic Tool in AnemiasDokumen4 halamanRBC Histogram As Diagnostic Tool in AnemiasIOSRjournalBelum ada peringkat
- Menejeman LabDokumen3 halamanMenejeman LabElvan Dwi WidyadiBelum ada peringkat
- Journal of Global Pharma Technology: Research PaperDokumen5 halamanJournal of Global Pharma Technology: Research PaperItyn MohamadBelum ada peringkat
- Main Article - BM PancytopeniaDokumen10 halamanMain Article - BM PancytopeniaAbdur Rachman Ba'abdullahBelum ada peringkat
- Pjms 29 1153Dokumen5 halamanPjms 29 1153Hanshel SatriyaBelum ada peringkat
- 4489 18254 1 PBDokumen4 halaman4489 18254 1 PBivanBelum ada peringkat
- Clinical Manifestation in Sickle Cell Anemia: A Study in Chhattisgarh Institute of Medical Sciences (CIMS) Bilaspur, Chhattisgarh, India.Dokumen4 halamanClinical Manifestation in Sickle Cell Anemia: A Study in Chhattisgarh Institute of Medical Sciences (CIMS) Bilaspur, Chhattisgarh, India.IOSRjournalBelum ada peringkat
- Levels of Markers of Myocardial Infarction and Atherogenicity in Individuals With Sickle Cell TraitDokumen6 halamanLevels of Markers of Myocardial Infarction and Atherogenicity in Individuals With Sickle Cell TraitKIU PUBLICATION AND EXTENSIONBelum ada peringkat
- Validation Biochemistry MeasurementDokumen35 halamanValidation Biochemistry Measurementhudan aziziBelum ada peringkat
- Full Blood Count Apr04, DR Eva RaikDokumen7 halamanFull Blood Count Apr04, DR Eva RaikDanielcc LeeBelum ada peringkat
- JCM 08 01175 v2 PDFDokumen28 halamanJCM 08 01175 v2 PDFAs'har AnwarBelum ada peringkat
- Toward 21st Century Blood Component Replacement Therapeutics: Artificial Oxygen Carriers, Platelet Substitutes, Recombinant Clotting Factors, and OthersDokumen15 halamanToward 21st Century Blood Component Replacement Therapeutics: Artificial Oxygen Carriers, Platelet Substitutes, Recombinant Clotting Factors, and OthersIstván PortörőBelum ada peringkat
- Hematological Parameters and Prevalence of Anemia Among Free-Living Elderly in South BrazilDokumen4 halamanHematological Parameters and Prevalence of Anemia Among Free-Living Elderly in South BrazilEmy YulianaBelum ada peringkat
- Vitamin B12 Pancytopneia RecorrectedDokumen8 halamanVitamin B12 Pancytopneia RecorrectedSafdar Shabir AwanBelum ada peringkat
- Laboratory Features of Systemic Lupus Erythematosus (SLE)Dokumen6 halamanLaboratory Features of Systemic Lupus Erythematosus (SLE)AmrKamalBelum ada peringkat
- Literature Review On Sickle Cell DiseaseDokumen8 halamanLiterature Review On Sickle Cell Diseaseafmzwflmdnxfeb100% (1)
- 31 Pankaj EtalDokumen3 halaman31 Pankaj EtaleditorijmrhsBelum ada peringkat
- 2007 28 259 M. Catherine Driscoll: Pediatrics in ReviewDokumen12 halaman2007 28 259 M. Catherine Driscoll: Pediatrics in ReviewcharlesBelum ada peringkat
- 1833 Manuscript 7430 1 10 20180428Dokumen6 halaman1833 Manuscript 7430 1 10 20180428sagarBelum ada peringkat
- 1 Ajaz 2012Dokumen4 halaman1 Ajaz 2012Olivia Valentine LekiBelum ada peringkat
- Complementary and Alternative Medical Lab Testing Part 16: HematologyDari EverandComplementary and Alternative Medical Lab Testing Part 16: HematologyBelum ada peringkat
- Nej Me 1204395Dokumen2 halamanNej Me 1204395Ferdy SetiawanBelum ada peringkat
- Use of Blood Product in SepsisDokumen6 halamanUse of Blood Product in SepsisAditya IrawanBelum ada peringkat
- Clinical Cases: World Journal ofDokumen8 halamanClinical Cases: World Journal ofhoude zhangBelum ada peringkat
- Queries - RBC DisordersDokumen14 halamanQueries - RBC DisordersHello PBJBelum ada peringkat
- ThalassemiaminorDokumen5 halamanThalassemiaminorAndreaFonsecaBelum ada peringkat
- Hodgkin LyphomaDokumen6 halamanHodgkin LyphomaJose Luis PittauBelum ada peringkat
- HemeoncalgorithmsDokumen11 halamanHemeoncalgorithmsida ayu agung WijayantiBelum ada peringkat
- Summary of Summary 5Dokumen36 halamanSummary of Summary 5anon-265120100% (2)
- Blood 2012 Allen 2939 44Dokumen7 halamanBlood 2012 Allen 2939 44Imam MuliaBelum ada peringkat
- Thesis On Beta ThalassemiaDokumen6 halamanThesis On Beta ThalassemiaBuyingPapersForCollegeUK100% (1)
- Comparative Evaluation of Blood Parameters in Chronic Periodontitis Patients and Healthy Patients For Signs of AnemiaDokumen7 halamanComparative Evaluation of Blood Parameters in Chronic Periodontitis Patients and Healthy Patients For Signs of AnemiaInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- 444 FullDokumen2 halaman444 FulllukbarniBelum ada peringkat
- Sickle Cell Anemia A Succinct Look Into Recently Tested Disease Modifying InterventionsDokumen10 halamanSickle Cell Anemia A Succinct Look Into Recently Tested Disease Modifying InterventionsAthenaeum Scientific PublishersBelum ada peringkat
- A Review of Electrophoretic Patterns From A Tertiary Care Nephrourology Referral CentreDokumen5 halamanA Review of Electrophoretic Patterns From A Tertiary Care Nephrourology Referral CentreTrương Ngọc HàBelum ada peringkat
- Clinico Hematological Profile of Hereditary Spherocytosis Experience From A Tertiary Care Center in North IndiaDokumen5 halamanClinico Hematological Profile of Hereditary Spherocytosis Experience From A Tertiary Care Center in North IndiaShafaque IrfanBelum ada peringkat
- 1 s2.0 S0168827804905533 MainDokumen1 halaman1 s2.0 S0168827804905533 Maindjafer maryaBelum ada peringkat
- BMED - Lab ReportDokumen7 halamanBMED - Lab ReportDaniella Stevanato SanchezBelum ada peringkat
- A Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarDokumen9 halamanA Clinicohaematological Profile of Splenomegaly: Varsha S. Dabadghao, Arundhati G.Diwan, Amol M. RaskarLianSiahaanBelum ada peringkat
- Marcus 1997Dokumen7 halamanMarcus 1997Araceli Enríquez OvandoBelum ada peringkat
- Survival Analysis in RDokumen8 halamanSurvival Analysis in RRobert DwitamaBelum ada peringkat
- 1768 PDFDokumen2 halaman1768 PDFAndhiky Raymonanda MadangsaiBelum ada peringkat
- Jurnal 5Dokumen4 halamanJurnal 5Ciendy ShintyaBelum ada peringkat
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDokumen5 halaman"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDokumen7 halamanSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDokumen5 halamanAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDokumen7 halamanA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Dokumen15 halamanA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Belum ada peringkat
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDokumen6 halamanThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- The Impact of Technologies On Society: A ReviewDokumen5 halamanThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDokumen14 halamanAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Assessment of The Implementation of Federal Character in Nigeria.Dokumen5 halamanAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Belum ada peringkat
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDokumen7 halamanComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDokumen5 halamanEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDokumen4 halamanInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDokumen5 halamanRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Importance of Mass Media in Communicating Health Messages: An AnalysisDokumen6 halamanImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Role of Madarsa Education in Empowerment of Muslims in IndiaDokumen6 halamanRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDokumen7 halamanTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDokumen5 halamanDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalBelum ada peringkat
- 1P 2 OB1-Maternal-AnatomyDokumen11 halaman1P 2 OB1-Maternal-AnatomyGeevee Naganag VentulaBelum ada peringkat
- Human Body Parts and OrgansDokumen2 halamanHuman Body Parts and OrgansRobbie Ac100% (1)
- CRPSDokumen8 halamanCRPSchinmayghaisasBelum ada peringkat
- Meridian /channel: Simplified Chinese Traditional Chinese PinyinDokumen20 halamanMeridian /channel: Simplified Chinese Traditional Chinese Pinyinramesh2007-mptBelum ada peringkat
- Lesson 1 "Modern Health Problems": A. Before-Reading ActivitiesDokumen3 halamanLesson 1 "Modern Health Problems": A. Before-Reading ActivitiesRomantische BohemienBelum ada peringkat
- Hot and Cold Therapy For SprainDokumen2 halamanHot and Cold Therapy For SprainJef BarrettBelum ada peringkat
- Mecanismos de Accion InotropicosDokumen8 halamanMecanismos de Accion InotropicosPaola DiazBelum ada peringkat
- PG 0471Dokumen1 halamanPG 0471MihaelaBelum ada peringkat
- Exercise 6 Frog Embryology - 1Dokumen10 halamanExercise 6 Frog Embryology - 1ANNE MARGUERITE BARETEBelum ada peringkat
- Vomiting: Compendium (Yardley, PA) February 2009Dokumen10 halamanVomiting: Compendium (Yardley, PA) February 2009Vini SasmitaBelum ada peringkat
- Anatomy of LungsDokumen4 halamanAnatomy of Lungs31 PASION, ROCHELLE C.Belum ada peringkat
- Drug Study HydralazineDokumen10 halamanDrug Study HydralazineLuige AvilaBelum ada peringkat
- No Way Out of The Binary: A Critical History of The Scientific Production of SexDokumen27 halamanNo Way Out of The Binary: A Critical History of The Scientific Production of SexCeciliaRustoBelum ada peringkat
- Auricular Acupuncture 2013 SummerDokumen89 halamanAuricular Acupuncture 2013 Summerdoringrama100% (3)
- Treatment of Central Sleep Apnea With Adaptive Servoventilation in Chronic Heart FailureDokumen3 halamanTreatment of Central Sleep Apnea With Adaptive Servoventilation in Chronic Heart Failureerwanrispandi03Belum ada peringkat
- Pulling Er 2013Dokumen23 halamanPulling Er 2013Diana Margarita EcheverriBelum ada peringkat
- Important Question For Dialysis TechnicianDokumen7 halamanImportant Question For Dialysis Technicianhunbaitmiki hinge100% (1)
- Behaviours Learned Through Classical ConditioningDokumen6 halamanBehaviours Learned Through Classical Conditioningapi-314561050Belum ada peringkat
- Cell Organelles Webquest Day 2 With Notes Filled inDokumen3 halamanCell Organelles Webquest Day 2 With Notes Filled inJustin TisBelum ada peringkat
- Answer Key Simulated Pre Board Set 4 NagaDokumen11 halamanAnswer Key Simulated Pre Board Set 4 NagaRaymark MoralesBelum ada peringkat
- PAPER (ENG) - Pseudodysphagia Due To Omohyoid Muscle SyndromeDokumen6 halamanPAPER (ENG) - Pseudodysphagia Due To Omohyoid Muscle SyndromeAldo Hip NaranjoBelum ada peringkat
- Low Back Pain SlidesDokumen27 halamanLow Back Pain SlidesAviv Aziz Triono100% (1)
- Epithelial TissueDokumen11 halamanEpithelial TissueFadhil Hussam AhmedBelum ada peringkat
- Turner HypoplasiaDokumen5 halamanTurner HypoplasiaAzi Pertiwi HussainBelum ada peringkat
- Sphaerotilus NDokumen2 halamanSphaerotilus NLuis M. Telleria CondeBelum ada peringkat
- Makalah Sistem Pencernaan Bhs InggrisDokumen32 halamanMakalah Sistem Pencernaan Bhs InggrisDesiBelum ada peringkat
- Psych 372 S'22 Study Guide For QUIZZES 1-3 & EXAM 1Dokumen4 halamanPsych 372 S'22 Study Guide For QUIZZES 1-3 & EXAM 1darby hepplerBelum ada peringkat
- Barra FixaDokumen11 halamanBarra FixaMarcos AndréBelum ada peringkat