Anda mungkin juga menyukai
- Ford Taurus Service Manual - Disassembly and Assembly - Automatic Transaxle-Transmission - 6F35 - Automatic Transmission - PowertrainDokumen62 halamanFord Taurus Service Manual - Disassembly and Assembly - Automatic Transaxle-Transmission - 6F35 - Automatic Transmission - Powertraininfocarsservice.deBelum ada peringkat
- Principles of The Doctrine of ChristDokumen17 halamanPrinciples of The Doctrine of ChristNovus Blackstar100% (2)
- BC C Punmia BeamDokumen14 halamanBC C Punmia BeamvikrantgoudaBelum ada peringkat
- Introduction To Wireless Communication - Radio CommunicationDokumen21 halamanIntroduction To Wireless Communication - Radio CommunicationYas773Belum ada peringkat
- Instruction Manual for Capacitor Voltage TransformersDokumen22 halamanInstruction Manual for Capacitor Voltage Transformerst.o.i.n.gBelum ada peringkat
- Komatsu HD785-7 Shop Manual PDFDokumen1.491 halamanKomatsu HD785-7 Shop Manual PDFIB EldinBelum ada peringkat
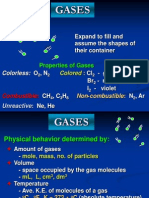
- Properties and Behavior of GasesDokumen34 halamanProperties and Behavior of GasesPaul Jeremiah Serrano NarvaezBelum ada peringkat
- Record of Appropriations and Obligations: TotalDokumen1 halamanRecord of Appropriations and Obligations: TotaljomarBelum ada peringkat
- YavorskyDokumen544 halamanYavorskyFilipe PadilhaBelum ada peringkat
- Differential Scanning CalorimetryDokumen60 halamanDifferential Scanning CalorimetryMariyam100% (2)
- Hunch or Reason?: Reading File 11Dokumen2 halamanHunch or Reason?: Reading File 11georgiana dinuBelum ada peringkat
- Association Between Alcohol Consumption and Hypertension: Myoung Kyun Son, MDDokumen9 halamanAssociation Between Alcohol Consumption and Hypertension: Myoung Kyun Son, MDAlessandraBelum ada peringkat
- Hypertension Prevalence, Awareness, Control and Association With Metabolic Abnormalities in The San Marino Population: The SMOOTH StudyDokumen7 halamanHypertension Prevalence, Awareness, Control and Association With Metabolic Abnormalities in The San Marino Population: The SMOOTH StudyIndah SundariBelum ada peringkat
- Alcohol 5Dokumen6 halamanAlcohol 5Enayet Karim ChowdhuryBelum ada peringkat
- The Relation of Moderate Alcohol Consumption To Hyperuricemia in A Rural General PopulationDokumen11 halamanThe Relation of Moderate Alcohol Consumption To Hyperuricemia in A Rural General PopulationsyifaBelum ada peringkat
- Nutrition Parameters As Hemodialysis Adequacy Markers: Original ArticleDokumen5 halamanNutrition Parameters As Hemodialysis Adequacy Markers: Original ArticleMariska Widya WBelum ada peringkat
- Gupea 2077 35191 1Dokumen81 halamanGupea 2077 35191 1pearl ikebuakuBelum ada peringkat
- MJMHS 0513Dokumen10 halamanMJMHS 0513aisha.alhamadi99Belum ada peringkat
- Urban-Rural Disease Its Factors: Differences in The Prevalence of Coronary Heart and Risk in DelhiDokumen8 halamanUrban-Rural Disease Its Factors: Differences in The Prevalence of Coronary Heart and Risk in DelhiputiridhaBelum ada peringkat
- Association Between Health Literacy and Hypertension Management in A Chinese Community: A Retrospective Cohort StudyDokumen12 halamanAssociation Between Health Literacy and Hypertension Management in A Chinese Community: A Retrospective Cohort StudyDwikani Oklita AnggirulingBelum ada peringkat
- Hypertension ThesisDokumen31 halamanHypertension ThesisNavin AdhikariBelum ada peringkat
- Bmjopen 2016 014736Dokumen6 halamanBmjopen 2016 014736puskesmas patuk satuBelum ada peringkat
- High Blood Pressure and The Measures To Prevent Cardiovascular Disease of HypertensionDokumen4 halamanHigh Blood Pressure and The Measures To Prevent Cardiovascular Disease of HypertensionEto ShengeliaBelum ada peringkat
- Smoking and Blood Sugar Linked to Cardiovascular RiskDokumen11 halamanSmoking and Blood Sugar Linked to Cardiovascular Riskinflibnet inflibnetBelum ada peringkat
- Interheart FinalDokumen55 halamanInterheart FinalRajeev Chugh75% (4)
- TMKDokumen7 halamanTMKDanu Satria OBelum ada peringkat
- Park K & Kim K, 2012Dokumen6 halamanPark K & Kim K, 2012syifaBelum ada peringkat
- 302 Cardiovascular Risk: AssessmentDokumen1 halaman302 Cardiovascular Risk: AssessmentLêHữuHoàiBelum ada peringkat
- Relation Between Vascular Risk Factors and Cognition at Age 75Dokumen7 halamanRelation Between Vascular Risk Factors and Cognition at Age 75Fajar Rudy QimindraBelum ada peringkat
- Serum Taurine and Risk of Coronary Heart Disease: A Prospective, Nested Case-Control StudyDokumen10 halamanSerum Taurine and Risk of Coronary Heart Disease: A Prospective, Nested Case-Control StudyThalia KarampasiBelum ada peringkat
- Sahle 2018Dokumen7 halamanSahle 2018Ester DuwitBelum ada peringkat
- Prehypertensive and Mildly Hypertensive Young Adults at Higher Cardiovascular RiskDokumen8 halamanPrehypertensive and Mildly Hypertensive Young Adults at Higher Cardiovascular RiskIndah SundariBelum ada peringkat
- Reiki Therapy Reduces HypertensionDokumen34 halamanReiki Therapy Reduces HypertensionYayu AlawiiahBelum ada peringkat
- Epidemiology of The Metabolic Syndrome in Hungary: Public HealthDokumen7 halamanEpidemiology of The Metabolic Syndrome in Hungary: Public Healthadi suputraBelum ada peringkat
- FrancoisDokumen13 halamanFrancoismufti dewantaraBelum ada peringkat
- Family Member-Based Supervision of Patients With Hypertension: A Cluster Randomized Trial in Rural ChinaDokumen8 halamanFamily Member-Based Supervision of Patients With Hypertension: A Cluster Randomized Trial in Rural ChinaAchmad YasinBelum ada peringkat
- The TEPHRA Trial Is The First Study With The Primary Aim of Determining The Effects of Structured Aerobic Exercise and Physical Activity SelfDokumen9 halamanThe TEPHRA Trial Is The First Study With The Primary Aim of Determining The Effects of Structured Aerobic Exercise and Physical Activity Selfach maskurBelum ada peringkat
- Dose-Response Association of Uncontrolled Blood Pressure and Cardiovascular Disease Risk Factors With Hyperuricemia and GoutDokumen8 halamanDose-Response Association of Uncontrolled Blood Pressure and Cardiovascular Disease Risk Factors With Hyperuricemia and GoutxoxotheBelum ada peringkat
- Effect of BmiDokumen5 halamanEffect of BmiSyaiful Putra RanaBelum ada peringkat
- The Prevalence of ArterialDokumen8 halamanThe Prevalence of ArterialInternational Medical PublisherBelum ada peringkat
- Combined Effects of Smoking and Systolic Blood Pressure On Risk of Coronary Heart Disease: A Cohort Study in Chinese WomenDokumen7 halamanCombined Effects of Smoking and Systolic Blood Pressure On Risk of Coronary Heart Disease: A Cohort Study in Chinese Womenb10879832Belum ada peringkat
- Blood Pressure, Serum Total Cholesterol and Contraceptive Pill Use in 17-Year-Old GirlsDokumen5 halamanBlood Pressure, Serum Total Cholesterol and Contraceptive Pill Use in 17-Year-Old GirlsLucerito MartinezBelum ada peringkat
- Alkohol 2Dokumen10 halamanAlkohol 2Yuvhendmindo ShahcogaBelum ada peringkat
- Assessment of Overweight and High Blood Pressure Among Individuals in Out - Patient Clinic in A Specialist HospitalDokumen3 halamanAssessment of Overweight and High Blood Pressure Among Individuals in Out - Patient Clinic in A Specialist HospitalIOSRjournalBelum ada peringkat
- Joint Effect of Cigarette Smoking and Body Mass Index On White Blood Cell Count in Korean AdultsDokumen6 halamanJoint Effect of Cigarette Smoking and Body Mass Index On White Blood Cell Count in Korean AdultsajBelum ada peringkat
- E2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Dokumen1 halamanE2 Journal of Hypertension Vol 35, E-Supplement 3, November 2017Sadam_fasterBelum ada peringkat
- PHSC 100 Research Paper - IsrarDokumen17 halamanPHSC 100 Research Paper - IsrarAhmer IsrarBelum ada peringkat
- Sex-Related Relationships Between Uric Acid AnDokumen8 halamanSex-Related Relationships Between Uric Acid Annguyenthanhluan2801Belum ada peringkat
- Proton-Pump Inhibitors Therapy and Blood Pressure ControlDokumen6 halamanProton-Pump Inhibitors Therapy and Blood Pressure ControlTeky WidyariniBelum ada peringkat
- Nje 05 480Dokumen8 halamanNje 05 480Gilang Nesta PersempreBelum ada peringkat
- The Effectiveness of Intensive Nursing Care On Seasonal Variation of Blood Pressure in Patients On Peritoneal DialysisDokumen10 halamanThe Effectiveness of Intensive Nursing Care On Seasonal Variation of Blood Pressure in Patients On Peritoneal DialysisBaeyou MennongBelum ada peringkat
- Association Between Sugar-Sweetened Beverage Consumption and Incident Hypertension in Korean Adults: A Prospective StudyDokumen9 halamanAssociation Between Sugar-Sweetened Beverage Consumption and Incident Hypertension in Korean Adults: A Prospective StudyDwikani Oklita AnggirulingBelum ada peringkat
- Materials and MethodsDokumen5 halamanMaterials and Methodsike ikeBelum ada peringkat
- Patient Prefer AdherenceDokumen35 halamanPatient Prefer Adherencearriane_rosalesBelum ada peringkat
- Postdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityDokumen6 halamanPostdialysis Hypertension: Associated Factors, Patient Profiles, and Cardiovascular MortalityLaura PutriBelum ada peringkat
- Nejmoa 032782Dokumen10 halamanNejmoa 032782elvinegunawanBelum ada peringkat
- The Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsDokumen9 halamanThe Efficacy and Safety of Triple Vs Dual Combination of ARB, CCB, and DiureticsLucky PratamaBelum ada peringkat
- 28xlekosit Between Diabetes Complications LekositDokumen5 halaman28xlekosit Between Diabetes Complications LekositHoopmen tampubolonBelum ada peringkat
- Obesitas 2 ObesitasDokumen14 halamanObesitas 2 ObesitasJeremy KerrBelum ada peringkat
- Association of High Blood Pressure With RenalDokumen6 halamanAssociation of High Blood Pressure With RenalBima AryaputraBelum ada peringkat
- Clinical Study: The Association Between Intradialytic Hypertension and Metabolic Disorders in End Stage Renal DiseaseDokumen9 halamanClinical Study: The Association Between Intradialytic Hypertension and Metabolic Disorders in End Stage Renal Diseasecynthia nataliaBelum ada peringkat
- Among Hypertensive PatientDokumen26 halamanAmong Hypertensive PatientRam ChandranBelum ada peringkat
- Estudo CompletoDokumen16 halamanEstudo CompletoRitaIvoBelum ada peringkat
- Paper Seminar English 1Dokumen6 halamanPaper Seminar English 1Neva JudhantiBelum ada peringkat
- Analysis of Blood Glucose Distribution Characteristics and Its Risk Factors Among A Health Examination Population in Wuhu (China)Dokumen9 halamanAnalysis of Blood Glucose Distribution Characteristics and Its Risk Factors Among A Health Examination Population in Wuhu (China)Aleksa CopicBelum ada peringkat
- Epidemiology of Hypertension and Metabolic Disorders: 10.1016/j.ijcard.2011.08.581Dokumen2 halamanEpidemiology of Hypertension and Metabolic Disorders: 10.1016/j.ijcard.2011.08.581Mirza RisqaBelum ada peringkat
- Sectional, Pemilihan Sampel Dengan Purposive Sampling. Sampel 72 Responden. PengumpulanDokumen8 halamanSectional, Pemilihan Sampel Dengan Purposive Sampling. Sampel 72 Responden. PengumpulandanuBelum ada peringkat
- Blood Pressure Difference Between Pre and PostDokumen3 halamanBlood Pressure Difference Between Pre and PostObada AlsadeqBelum ada peringkat
- Chan Et Al (2000)Dokumen6 halamanChan Et Al (2000)badrishBelum ada peringkat
- The Determinants of Hypertension Awareness, Treatment, and Control in An Insured PopulationDokumen7 halamanThe Determinants of Hypertension Awareness, Treatment, and Control in An Insured PopulationHugo Suarez RomeroBelum ada peringkat
- Complementary and Alternative Medical Lab Testing Part 4: VascularDari EverandComplementary and Alternative Medical Lab Testing Part 4: VascularBelum ada peringkat
- Lembar LPDokumen2 halamanLembar LPDyan TDBelum ada peringkat
- Minee WebDokumen1 halamanMinee Webmasykur_aliyBelum ada peringkat
- Minee WebDokumen1 halamanMinee Webmasykur_aliyBelum ada peringkat
- Drug use questionnaire scoring guideDokumen2 halamanDrug use questionnaire scoring guideMuhammad FarhanBelum ada peringkat
- 841 1668 1 SMDokumen1 halaman841 1668 1 SMDyan TDBelum ada peringkat
- Hepti Muliyati, Aminuddin Syam, Saifuddin Sirajuddin: Artikel PenelitianDokumen7 halamanHepti Muliyati, Aminuddin Syam, Saifuddin Sirajuddin: Artikel PenelitianHermansyah ChiuBelum ada peringkat
- 1471 2261 12 88Dokumen6 halaman1471 2261 12 88Dyan TDBelum ada peringkat
- Tamponade JantungDokumen4 halamanTamponade JantungDyan TDBelum ada peringkat
- Pediatrics 2005 Shipley 1150 7Dokumen10 halamanPediatrics 2005 Shipley 1150 7Dyan TDBelum ada peringkat
- Fluid BalanceCorr PDFDokumen5 halamanFluid BalanceCorr PDFSu'ud DeLoco's100% (1)
- Wound Care Skills Checklist: Work SettingsDokumen3 halamanWound Care Skills Checklist: Work SettingsDyan TDBelum ada peringkat
- Fluid BalanceCorr PDFDokumen5 halamanFluid BalanceCorr PDFSu'ud DeLoco's100% (1)
- How To Choose The Appropriate DressingDokumen4 halamanHow To Choose The Appropriate DressingDyan TD100% (1)
- Red Lion MP Sensor Product Manual PDFDokumen2 halamanRed Lion MP Sensor Product Manual PDFJigneshBelum ada peringkat
- (Homebrew) ShamanDokumen15 halaman(Homebrew) ShamanVictor Wanderley CorrêaBelum ada peringkat
- Bill Porter Updated PDFDokumen3 halamanBill Porter Updated PDFapi-362500677Belum ada peringkat
- Mr. Sanjeev Nanda - Devoted Son and GrandsonDokumen1 halamanMr. Sanjeev Nanda - Devoted Son and GrandsonSanjeev NandaBelum ada peringkat
- Understanding the Difference Between Positive and Normative EconomicsDokumen21 halamanUnderstanding the Difference Between Positive and Normative EconomicsKevin Fernandez MendioroBelum ada peringkat
- Educational PlanningDokumen20 halamanEducational PlanningedelynBelum ada peringkat
- Communication Thesis PDFDokumen2 halamanCommunication Thesis PDFBarbara0% (2)
- 2015 StoneAge - LowresDokumen51 halaman2015 StoneAge - LowresAZLAN ABDULLAIBelum ada peringkat
- Virtual Art PaperDokumen5 halamanVirtual Art Paperbrandy oldfieldBelum ada peringkat
- Life and Works or Rizal - EssayDokumen2 halamanLife and Works or Rizal - EssayQuince CunananBelum ada peringkat
- TLC Treatment and Marketing ProposalDokumen19 halamanTLC Treatment and Marketing Proposalbearteddy17193Belum ada peringkat
- ADEC Al Maali International Private School 2015 2016Dokumen18 halamanADEC Al Maali International Private School 2015 2016Edarabia.com100% (1)
- Tauros TBM Guidance SystemDokumen3 halamanTauros TBM Guidance SystemMiloš StanimirovićBelum ada peringkat
- Oracle Fusion Middleware: CloningDokumen25 halamanOracle Fusion Middleware: CloningSwathiPatluriBelum ada peringkat
- DHRM 3 SyllabusDokumen10 halamanDHRM 3 SyllabusCherokee Tuazon RodriguezBelum ada peringkat
- Cronbach AlphaDokumen15 halamanCronbach AlphaRendy EdistiBelum ada peringkat
- 4.6.6 Lab View Wired and Wireless Nic InformationDokumen4 halaman4.6.6 Lab View Wired and Wireless Nic InformationThắng NguyễnBelum ada peringkat
- Material For Werable AntennaDokumen4 halamanMaterial For Werable AntennaMujeeb AbdullahBelum ada peringkat
- Ozone Layer EssayDokumen7 halamanOzone Layer Essayb71bpjha100% (2)