Anda mungkin juga menyukai
- Flyer Asmpid 2021Dokumen2 halamanFlyer Asmpid 2021Agus WijataBelum ada peringkat
- Nna en November09Dokumen3 halamanNna en November09Agus WijataBelum ada peringkat
- Kids Games Powerpoint TemplateDokumen26 halamanKids Games Powerpoint TemplateAgus WijataBelum ada peringkat
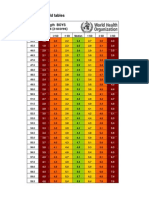
- WHO New Zscore WLZ Boys 0-2yrsDokumen5 halamanWHO New Zscore WLZ Boys 0-2yrsAgus WijataBelum ada peringkat
- Status of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaDokumen4 halamanStatus of Serum Bilirubin, Serum Proteins and Prothrombin Time in Babies With Perinatal AsphyxiaAgus WijataBelum ada peringkat
- Early Biochemical Indicators of Hypoxic-Ischemic Encephalopathy After Birth AsphyxiaDokumen5 halamanEarly Biochemical Indicators of Hypoxic-Ischemic Encephalopathy After Birth AsphyxiaAgus WijataBelum ada peringkat
- Espr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedDokumen1 halamanEspr Abstracts: Background: Hypoxic-Ischemic Brain Injury (HIE) Is The Most Common Perinatal Cerebral Insult AssociatedAgus WijataBelum ada peringkat
- KBM0701 Stern 21Dokumen6 halamanKBM0701 Stern 21Agus WijataBelum ada peringkat
- Biochemical Marker As Predictor of Outcome in Perinatal AsphyxiaDokumen4 halamanBiochemical Marker As Predictor of Outcome in Perinatal AsphyxiaAgus WijataBelum ada peringkat
- Edwin Kim, MD A. Wesley Burks, MD Michael Pistiner, MD, MMSCDokumen1 halamanEdwin Kim, MD A. Wesley Burks, MD Michael Pistiner, MD, MMSCAgus WijataBelum ada peringkat
- Neuron-Specific Enolase As A Marker of The Severity and Outcome of Hypoxic Ischemic EncephalopathyDokumen5 halamanNeuron-Specific Enolase As A Marker of The Severity and Outcome of Hypoxic Ischemic EncephalopathyAgus WijataBelum ada peringkat
- MML Test Setup PDFDokumen1 halamanMML Test Setup PDFAgus WijataBelum ada peringkat
- Bloody DDokumen31 halamanBloody DAgus WijataBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Flowchart For Drug Surrender: Pnp/PdeaDokumen2 halamanFlowchart For Drug Surrender: Pnp/PdeaLuppo PcaduBelum ada peringkat
- Vaccines and Medicines of Pets in PakistanDokumen7 halamanVaccines and Medicines of Pets in PakistanTress Lavena100% (1)
- Assessing Cognitive Impairment in Patients With SchizophreniaDokumen5 halamanAssessing Cognitive Impairment in Patients With SchizophreniaShifa TifarinBelum ada peringkat
- Health Insurance in India-An Overview: K.Swathi, R.AnuradhaDokumen4 halamanHealth Insurance in India-An Overview: K.Swathi, R.AnuradhaAnkit YadavBelum ada peringkat
- Ventricular Aneurysm: PathophysiologyDokumen3 halamanVentricular Aneurysm: PathophysiologyMegan N. ReyesBelum ada peringkat
- Original PDF Clinical Experiences in Counseling by Bradley T Erford PDFDokumen41 halamanOriginal PDF Clinical Experiences in Counseling by Bradley T Erford PDFwillie.dorich827100% (37)
- LESSON PLAN - AnagicisDokumen22 halamanLESSON PLAN - AnagicisrenuBelum ada peringkat
- Sample I-Search Paper 2014Dokumen7 halamanSample I-Search Paper 2014univfi12100% (3)
- Fundamentals of NursingDokumen268 halamanFundamentals of Nursinguhta100% (1)
- Materi Dokter Bayu TGL 9 Juli 2020Dokumen53 halamanMateri Dokter Bayu TGL 9 Juli 2020humaira noorBelum ada peringkat
- RRLDokumen12 halamanRRLEmilyne Joy Mendoza CabayaBelum ada peringkat
- ACSM's Complete Guide To Fitness & Health, 2nd EditionDokumen449 halamanACSM's Complete Guide To Fitness & Health, 2nd EditionRitaMata95% (22)
- Anal AbscessDokumen5 halamanAnal AbscessFernia StevaniBelum ada peringkat
- CN Mini ProjectDokumen5 halamanCN Mini ProjectA To Z INFOBelum ada peringkat
- Analisis Kesehatan Dan Keselamatan Kerja Pada Industri Furnitur Kayu Dengan Metode Job Safety AnalysisDokumen10 halamanAnalisis Kesehatan Dan Keselamatan Kerja Pada Industri Furnitur Kayu Dengan Metode Job Safety Analysisyendri putri febriyantiBelum ada peringkat
- Reccomendation Letter 2Dokumen2 halamanReccomendation Letter 2api-399482148Belum ada peringkat
- International Journal of Trend in Scientific Research and Development (IJTSRD)Dokumen5 halamanInternational Journal of Trend in Scientific Research and Development (IJTSRD)Editor IJTSRDBelum ada peringkat
- Chapter 7. 112 AffirmationsDokumen15 halamanChapter 7. 112 AffirmationsSharad PawarBelum ada peringkat
- Diass InfographicDokumen1 halamanDiass InfographicMichaer AmingBelum ada peringkat
- Certificate IV in Commercial Cookery Sit 40516Dokumen8 halamanCertificate IV in Commercial Cookery Sit 40516Tikaram GhimireBelum ada peringkat
- Surgical Nutrition: Vic V.Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryDokumen54 halamanSurgical Nutrition: Vic V.Vernenkar, D.O. St. Barnabas Hospital Dept. of SurgeryAmir SharifBelum ada peringkat
- A Reflection Paper On A Day in The Life of An Orthopedic NurseDokumen2 halamanA Reflection Paper On A Day in The Life of An Orthopedic NurseBernice EbbiBelum ada peringkat
- Safety Data Sheet: 1. Identification of The Substance/Preparation and of The Company/UndertakingDokumen6 halamanSafety Data Sheet: 1. Identification of The Substance/Preparation and of The Company/UndertakingJulion2009Belum ada peringkat
- The History of The Dentistry Con Correcciones (Martin Eduardo Rojas Ochoa)Dokumen2 halamanThe History of The Dentistry Con Correcciones (Martin Eduardo Rojas Ochoa)Maria Fernanda GarciaBelum ada peringkat
- Health Education Feb. 23, 2024Dokumen2 halamanHealth Education Feb. 23, 2024Ma. Jhysavil Arcena100% (1)
- Safety-Quality Apa PaperDokumen6 halamanSafety-Quality Apa Paperapi-241392518Belum ada peringkat
- Types of Hospitals: Gynecology Services & Other Facilities Pharmacy LaboratoryDokumen6 halamanTypes of Hospitals: Gynecology Services & Other Facilities Pharmacy LaboratoryMaham ShahidBelum ada peringkat
- Useful AbbreviationsDokumen2 halamanUseful AbbreviationsTracyBelum ada peringkat
- PretestDokumen3 halamanPretestcristy olivaBelum ada peringkat
- rd-15 Bartholin Cyst and Abscess 10-12 PDFDokumen2 halamanrd-15 Bartholin Cyst and Abscess 10-12 PDFdevidanthonyBelum ada peringkat