Anda mungkin juga menyukai
- Pilates AnatomyDokumen129 halamanPilates AnatomyAnkitBelum ada peringkat
- MAGEE - Avaliação Musculoesquelética - Testes EspeciaisDokumen468 halamanMAGEE - Avaliação Musculoesquelética - Testes EspeciaisCiro Albuquerque100% (11)
- Scapular Dyskinesis PDFDokumen24 halamanScapular Dyskinesis PDFPablo Sentis DiazBelum ada peringkat
- Manual Muscle TestingDokumen13 halamanManual Muscle TestingPásztai ZoltánBelum ada peringkat
- Frozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSDokumen6 halamanFrozen Shoulder - Adhesive Capsulitis - OrthoInfo - AAOSpempekplgBelum ada peringkat
- Kyphosis - Causes, Treatments & RisksDokumen8 halamanKyphosis - Causes, Treatments & Riskstarun72ceeBelum ada peringkat
- Physiomed Sitting Guide - Correct Sitting Posture Digital PDFDokumen12 halamanPhysiomed Sitting Guide - Correct Sitting Posture Digital PDFAdrian100% (1)
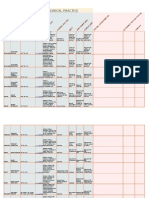
- Goniometry For Clinical PracticeDokumen7 halamanGoniometry For Clinical Practicedramitsaini33% (3)
- P.N.F Facial PalsyDokumen3 halamanP.N.F Facial PalsyUruchimaru100% (1)
- Sliders 3 HandbookDokumen23 halamanSliders 3 HandbookSean Price100% (2)
- Brachial Plexus InjuryDokumen59 halamanBrachial Plexus InjurySatya NagaraBelum ada peringkat
- Brachial Plexus SyndromesDokumen37 halamanBrachial Plexus SyndromesBruce Fredy Chino ChambillaBelum ada peringkat
- KyphosisDokumen32 halamanKyphosisBeniamin CostinașBelum ada peringkat
- Cap. 5 Kinesiology and Functional Characteristics of The Upper LimbDokumen30 halamanCap. 5 Kinesiology and Functional Characteristics of The Upper LimbLuis EstradaBelum ada peringkat
- Piriformissyndrome Exercise Sheet PDFDokumen2 halamanPiriformissyndrome Exercise Sheet PDFherikBelum ada peringkat
- GWS Total Hip ReplacementDokumen17 halamanGWS Total Hip ReplacementRadu MoglanBelum ada peringkat
- Scolio SIS: Submitted ToDokumen10 halamanScolio SIS: Submitted Tojean thereseBelum ada peringkat
- Rehabilitation of LeprosyDokumen72 halamanRehabilitation of LeprosyNur OctavianiBelum ada peringkat
- Erbs PalsyDokumen9 halamanErbs PalsyVatsalVermaBelum ada peringkat
- Common Shoulder Pathologies and Causes of Shoulder PainDokumen33 halamanCommon Shoulder Pathologies and Causes of Shoulder PainjermaineBelum ada peringkat
- Knee Replacement Exercises - NewDokumen2 halamanKnee Replacement Exercises - NewrBelum ada peringkat
- History of Spine BiomechanicsDokumen13 halamanHistory of Spine BiomechanicsLeopoldo AguayoBelum ada peringkat
- William C. Cottrell, MD AbstractDokumen4 halamanWilliam C. Cottrell, MD AbstractmalaBelum ada peringkat
- Evaluacion en OrtopediaDokumen7 halamanEvaluacion en OrtopediaFisio TerapiaBelum ada peringkat
- Chaptar 30 Degenerative Spine DiseaseDokumen9 halamanChaptar 30 Degenerative Spine DiseaseAbraham SaldañaBelum ada peringkat
- Physiotherapy After Hip HemiarthroplastyDokumen7 halamanPhysiotherapy After Hip HemiarthroplastyMellow Moon RecordsBelum ada peringkat
- Shoulder Impingement SyndromeDokumen21 halamanShoulder Impingement SyndromeivannaOctavianiBelum ada peringkat
- Hip Replacement GuideDokumen28 halamanHip Replacement GuideZulaika NaisBelum ada peringkat
- Biomechanics of The ElbowDokumen16 halamanBiomechanics of The ElbowAsmaa Ahmad SharawyBelum ada peringkat
- Physioterapy SalveDokumen45 halamanPhysioterapy SalveIkhar KeliobasBelum ada peringkat
- Anatomy of the Spine: Regions, Curves, and StructuresDokumen72 halamanAnatomy of the Spine: Regions, Curves, and StructuresMohammad Riedho Cahya AtazsuBelum ada peringkat
- Shoulder DislocationDokumen10 halamanShoulder DislocationStephanie AureliaBelum ada peringkat
- MGH Wrist and Elbow Strengthening ExercisesDokumen1 halamanMGH Wrist and Elbow Strengthening ExercisesRidwan Hadinata SalimBelum ada peringkat
- Nevralgia Cervico-BrahealaDokumen17 halamanNevralgia Cervico-BrahealaAlex RăşcanuBelum ada peringkat
- Total Knee Arthroplasty PDFDokumen10 halamanTotal Knee Arthroplasty PDFBhargav DaveBelum ada peringkat
- Shoulder Special TestDokumen2 halamanShoulder Special Testpandianshankar100% (1)
- Oswestry Disability IndexDokumen4 halamanOswestry Disability Indexpaulina_810Belum ada peringkat
- Genu Valgus Genu VarusDokumen35 halamanGenu Valgus Genu VarusRatu FaniaBelum ada peringkat
- Gait AnalysisDokumen6 halamanGait AnalysisryankelsallBelum ada peringkat
- Management of Flatfoot: The Best Foot ForwardDokumen40 halamanManagement of Flatfoot: The Best Foot Forwardshahalamkhan8914Belum ada peringkat
- Clavicle AO Surgery Reference (2023)Dokumen399 halamanClavicle AO Surgery Reference (2023)Wael GabrBelum ada peringkat
- Pathological GaitDokumen21 halamanPathological GaitGautham SridharBelum ada peringkat
- Shoulder Impigement ExercisesDokumen4 halamanShoulder Impigement ExercisesJörgen PuisBelum ada peringkat
- Can Trendelenburg'S Sign Be Positive If The Hip Is Normal?Dokumen5 halamanCan Trendelenburg'S Sign Be Positive If The Hip Is Normal?Juniarto PangestuBelum ada peringkat
- Williams Flexion Vs McKenzie Extension Exercises Low Back PainDokumen3 halamanWilliams Flexion Vs McKenzie Extension Exercises Low Back PainMasi KhanBelum ada peringkat
- Flatfoot Deformity An OverviewDokumen9 halamanFlatfoot Deformity An OverviewpetcudanielBelum ada peringkat
- Guidance and Guideline-Recommendations For The Treatment of Femoral Neck Fractures Romanian Society of Orthopaedics and Traumatology - SOROT 2018Dokumen8 halamanGuidance and Guideline-Recommendations For The Treatment of Femoral Neck Fractures Romanian Society of Orthopaedics and Traumatology - SOROT 2018Feny OktavianaBelum ada peringkat
- Brunnstorm ApproachDokumen70 halamanBrunnstorm Approachkomal khannaBelum ada peringkat
- C3-Evaluarea Motilitatii 2020Dokumen45 halamanC3-Evaluarea Motilitatii 2020Ovidiu MarianBelum ada peringkat
- Shoulder ArthroplastyDokumen53 halamanShoulder ArthroplastyWijaya X PutriBelum ada peringkat
- Theraex For IKFRDokumen130 halamanTheraex For IKFRsingle_ladyBelum ada peringkat
- Scoliosis: Degenerative & IdiopathicDokumen34 halamanScoliosis: Degenerative & IdiopathicClaudia MariscaBelum ada peringkat
- Bells PalsyDokumen66 halamanBells PalsyanshikaBelum ada peringkat
- Recuperare in AVCDokumen47 halamanRecuperare in AVCMarina IonescuBelum ada peringkat
- Wrist Complex1Dokumen25 halamanWrist Complex1bpt2100% (1)
- Orthotics and Prosthetics LectureDokumen40 halamanOrthotics and Prosthetics LectureRock Obaidat100% (1)
- Understanding brachial plexus injury diagnosis and treatment optionsDokumen48 halamanUnderstanding brachial plexus injury diagnosis and treatment optionsYoonHeeNyBelum ada peringkat
- Shoulder Anatomy & Biomechanics (Halder) PDFDokumen18 halamanShoulder Anatomy & Biomechanics (Halder) PDFNedelcuGeorgeBelum ada peringkat
- Kibler Scapular DyskinesisDokumen10 halamanKibler Scapular Dyskinesisנתנאל מושקוביץ100% (5)
- Brachial Plexus InjuryDokumen2 halamanBrachial Plexus InjuryRizal IsmuryandaBelum ada peringkat
- Brachial Plexus FAQsDokumen3 halamanBrachial Plexus FAQsandregomatBelum ada peringkat
- PALSYDokumen10 halamanPALSYGuhan SubramaniamBelum ada peringkat
- Erb'S Palsy: Definition/DescriptionDokumen10 halamanErb'S Palsy: Definition/DescriptionGuhan SubramaniamBelum ada peringkat
- Brachial Plexus InjuryDokumen10 halamanBrachial Plexus InjurySanditya FadliBelum ada peringkat
- Long Thoracic Nerve PalsyDokumen2 halamanLong Thoracic Nerve PalsyJose Luis Tabueña OrtegaBelum ada peringkat
- BrachialPlexus PDFDokumen1 halamanBrachialPlexus PDFKamran AfzalBelum ada peringkat
- Shiatsu: by Ciro Albuquerque IIDokumen23 halamanShiatsu: by Ciro Albuquerque IICiro AlbuquerqueBelum ada peringkat
- Brachial Plexus BookDokumen21 halamanBrachial Plexus BookCiro Albuquerque100% (1)
- Acupuncture For PhysiotherapistDokumen277 halamanAcupuncture For PhysiotherapistLuis Gomes100% (1)
- SLAP Lesion Repair Operation: A Guide For PatientsDokumen12 halamanSLAP Lesion Repair Operation: A Guide For PatientsCiro AlbuquerqueBelum ada peringkat
- UNIT I Movement EnhancementDokumen7 halamanUNIT I Movement EnhancementKervin Rey Guevarra JacksonBelum ada peringkat
- Stryker Shoulder ArthroplastyDokumen10 halamanStryker Shoulder Arthroplastymuhammad umarBelum ada peringkat
- Flexibility of SpineDokumen8 halamanFlexibility of SpinePawan Kumar YadavBelum ada peringkat
- CBSE Class 12 Physical Education Syllabus 2022 23Dokumen4 halamanCBSE Class 12 Physical Education Syllabus 2022 23aj singhBelum ada peringkat
- The Painful Shoulder: Part I. Clinical Evaluation - AAFPDokumen18 halamanThe Painful Shoulder: Part I. Clinical Evaluation - AAFPMelvin Florens Tania GongaBelum ada peringkat
- Push UpDokumen5 halamanPush UppavlocicBelum ada peringkat
- Module Description. Pathology of Musculosceletal SystemDokumen52 halamanModule Description. Pathology of Musculosceletal SystemAlberto MayorgaBelum ada peringkat
- 5 +Manual+Muscle+TestingDokumen36 halaman5 +Manual+Muscle+TestingMona AdjahBelum ada peringkat
- Anthropometric measurements for ergonomic designDokumen17 halamanAnthropometric measurements for ergonomic designTop Eleven2Belum ada peringkat
- Claw HandDokumen25 halamanClaw HandSunil Kumar PdBelum ada peringkat
- Protocolos LCADokumen8 halamanProtocolos LCAOmar VargasBelum ada peringkat
- Routines - GripTrainingDokumen23 halamanRoutines - GripTrainingRobert DEL POPOLO100% (1)
- Sacral OMM diagnosis and treatment techniquesDokumen4 halamanSacral OMM diagnosis and treatment techniquesSameer AkhtarBelum ada peringkat
- Normal Labor: Kevin Marcial I. Aralar, MD 1 Year ResidentDokumen46 halamanNormal Labor: Kevin Marcial I. Aralar, MD 1 Year ResidentKevin AralarBelum ada peringkat
- Managing Ankylosing Spondylitis in a 30-Year-Old MaleDokumen24 halamanManaging Ankylosing Spondylitis in a 30-Year-Old MaleDhieto Basuki PutraBelum ada peringkat
- Loki Man Level 1: 8 Phase Training 0 - IntermediateDokumen148 halamanLoki Man Level 1: 8 Phase Training 0 - IntermediateKathiravan KalidossBelum ada peringkat
- Range of Motion Exercise ChecklistDokumen3 halamanRange of Motion Exercise ChecklistSheená EspañolBelum ada peringkat
- Safran 2018Dokumen11 halamanSafran 2018Freddy ChurataBelum ada peringkat
- Radiculopatia CervicalDokumen8 halamanRadiculopatia CervicalFACIVERIBelum ada peringkat
- 1998 - Hawkey (Ankilosis y Discapacidad)Dokumen15 halaman1998 - Hawkey (Ankilosis y Discapacidad)Alejandro SernaBelum ada peringkat
- Bodybuilding - Weightlifting Training Database BookDokumen239 halamanBodybuilding - Weightlifting Training Database BookRavi Yalala100% (2)
- A Kinesiological Analysis of Shot BY WILLISDokumen16 halamanA Kinesiological Analysis of Shot BY WILLISNoraina AbdullahBelum ada peringkat
- Gross Anatomy CheatsheetDokumen302 halamanGross Anatomy CheatsheetNobody2015100% (1)
- Form RulaDokumen6 halamanForm RulaAndi MuliadiBelum ada peringkat
- OT 211 - Notes - IntroductionDokumen21 halamanOT 211 - Notes - Introductionno nameBelum ada peringkat