Anda mungkin juga menyukai
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Practice Exam - Qats PDFDokumen53 halamanPractice Exam - Qats PDFsdfbgshfgBelum ada peringkat
- S65 - Haldwani Lab Home Visit Haldwani: Patientreportscsuperpanel - SP - General - Template01 - SC (Version: 7)Dokumen2 halamanS65 - Haldwani Lab Home Visit Haldwani: Patientreportscsuperpanel - SP - General - Template01 - SC (Version: 7)rajasereddy1275Belum ada peringkat
- 2.4 & 2.5 Revision AnswersDokumen6 halaman2.4 & 2.5 Revision AnswersYuliya BoyalskayaBelum ada peringkat
- SDM Lab ReportDokumen3 halamanSDM Lab Reportapi-462451258Belum ada peringkat
- Feline Gastrointestinal Eosinofílica Fibroplasia EsclerosanteDokumen8 halamanFeline Gastrointestinal Eosinofílica Fibroplasia EsclerosanteCarlos Alberto Chaves VelasquezBelum ada peringkat
- Lymphoma and HIVDokumen20 halamanLymphoma and HIVALEX NAPOLEON CASTA�EDA SABOGAL100% (1)
- Systemic Infections From GiDokumen10 halamanSystemic Infections From GiJake MillerBelum ada peringkat
- Chapter 9 - Microbial ControlDokumen6 halamanChapter 9 - Microbial ControlAlicia Marie ElizaldeBelum ada peringkat
- Jackie Virology AssignmentDokumen6 halamanJackie Virology AssignmentDumisani NguniBelum ada peringkat
- Paper 2 November 2001Dokumen5 halamanPaper 2 November 2001MSHBelum ada peringkat
- Porphyria BJH Review PDFDokumen12 halamanPorphyria BJH Review PDFNexi anessaBelum ada peringkat
- TE Hepatitis B PD BUMILDokumen81 halamanTE Hepatitis B PD BUMILarrankBelum ada peringkat
- Bio1 11 - 12 Q1 0204 FDDokumen22 halamanBio1 11 - 12 Q1 0204 FDJoe Marc Lamosao CaninBelum ada peringkat
- Topic 8 - Grey MatterDokumen53 halamanTopic 8 - Grey MatterStudent 365Belum ada peringkat
- Chapter 4 The Sexual SelfDokumen13 halamanChapter 4 The Sexual SelfSherilyn Picarra100% (1)
- Polytene ChromosomesDokumen6 halamanPolytene ChromosomesKhush BakhtBelum ada peringkat
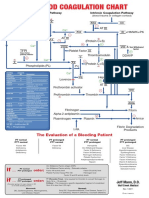
- Blood Clotting ChartDokumen1 halamanBlood Clotting ChartBianca SimionescuBelum ada peringkat
- 1.endo PerioLesionPartIThePathogenesisDokumen8 halaman1.endo PerioLesionPartIThePathogenesisMaulida SyafarinaBelum ada peringkat
- GI Tract InfectionsDokumen29 halamanGI Tract InfectionsMahrukh SiddiquiBelum ada peringkat
- PL - Patho 1.1 Theory NoteDokumen129 halamanPL - Patho 1.1 Theory Noteayusharya1303Belum ada peringkat
- Antibiotics ChartDokumen10 halamanAntibiotics ChartTrina Si100% (6)
- DAPI (4',6-Diamidine-2'-Phenylindole Dihydrochloride) : Cat. No. 10 236 276 001Dokumen2 halamanDAPI (4',6-Diamidine-2'-Phenylindole Dihydrochloride) : Cat. No. 10 236 276 001Estefani BlancasBelum ada peringkat
- Nitroimidazole Wps OfficeDokumen10 halamanNitroimidazole Wps OfficeCamelle DiniayBelum ada peringkat
- Upper Urinary Tract. InfectionDokumen11 halamanUpper Urinary Tract. InfectionnadhifBelum ada peringkat
- L04 - FC - Water and MoistureDokumen29 halamanL04 - FC - Water and MoistureEsteban RobayoBelum ada peringkat
- CMV Pregnancy 20Dokumen20 halamanCMV Pregnancy 20Татьяна ТутченкоBelum ada peringkat
- Cell Structures and FunctionsDokumen2 halamanCell Structures and FunctionsWallen LagradaBelum ada peringkat
- Plant Genome Projects PDFDokumen4 halamanPlant Genome Projects PDFmanoj_rkl_07100% (1)
- Proteins in Serum & UrineDokumen66 halamanProteins in Serum & Urinekiedd_04100% (1)
- ALK-positive Lung Cancer: A Moving TargetDokumen16 halamanALK-positive Lung Cancer: A Moving TargetcerbulcarpatinBelum ada peringkat