Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Daftar PustakaDokumen1 halamanDaftar PustakaTuti AlawiyahBelum ada peringkat
- Bab IDokumen42 halamanBab ITuti AlawiyahBelum ada peringkat
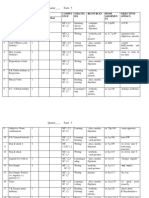
- Statistical Analysis: Table 1Dokumen6 halamanStatistical Analysis: Table 1Tuti AlawiyahBelum ada peringkat
- Daftar Hadir Departemen Neurologi FK Upn "Veteran" - Rsup Persahabatan Jakarta Periode 9 Februari 2015 - 14 Maret 2015 Minggu IDokumen3 halamanDaftar Hadir Departemen Neurologi FK Upn "Veteran" - Rsup Persahabatan Jakarta Periode 9 Februari 2015 - 14 Maret 2015 Minggu ITuti AlawiyahBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Human Resource Management StrategyDokumen41 halamanHuman Resource Management StrategymmzeeshanBelum ada peringkat
- 7th Grade - Exercise On HeatDokumen2 halaman7th Grade - Exercise On HeatBaiq Ayu ApriliaBelum ada peringkat
- Nurs 340 Group Process PaperDokumen7 halamanNurs 340 Group Process Paperapi-240550685Belum ada peringkat
- Largo, Johara D. FIDPDokumen4 halamanLargo, Johara D. FIDPJohara LargoBelum ada peringkat
- Grade 5...Dokumen19 halamanGrade 5...Nurkyz ZairovaBelum ada peringkat
- Ethics - Module 3Dokumen20 halamanEthics - Module 3Dale CalicaBelum ada peringkat
- Displaced Accents and PolyrhythmsDokumen2 halamanDisplaced Accents and PolyrhythmsJéssicaReisBelum ada peringkat
- Politeness Theory: by Brown and LavinsonDokumen3 halamanPoliteness Theory: by Brown and LavinsonBilingual CapriconBelum ada peringkat
- Reading Level of Grade 9 Male Students Chapter 1 5Dokumen43 halamanReading Level of Grade 9 Male Students Chapter 1 5Lala BolalaBelum ada peringkat
- 2nd Quarter EnglishDokumen26 halaman2nd Quarter EnglishAllan AlcantaraBelum ada peringkat
- From Gerrit KischnerDokumen6 halamanFrom Gerrit KischnerJulian A.Belum ada peringkat
- Unit 6 - WritingDokumen8 halamanUnit 6 - Writingtoannv8187Belum ada peringkat
- Araling Panlipunan Academic Festival Accomplishment ReportDokumen7 halamanAraling Panlipunan Academic Festival Accomplishment Reportlovely venia m jovenBelum ada peringkat
- Terjema, H 2.3.4.5.legal Research MethodsDokumen456 halamanTerjema, H 2.3.4.5.legal Research MethodsAlma AuliaBelum ada peringkat
- Work Ethics of The Proficient Teachers: Basis For A District Learning Action Cell (LAC) PlanDokumen11 halamanWork Ethics of The Proficient Teachers: Basis For A District Learning Action Cell (LAC) PlanJohn Giles Jr.Belum ada peringkat
- A Pragmatic Study of Yoruba Proverbs in English-90Dokumen10 halamanA Pragmatic Study of Yoruba Proverbs in English-90ednut_ynexBelum ada peringkat
- International Construction LawDokumen4 halamanInternational Construction LawSiso Castro LarsenBelum ada peringkat
- A Seventh Grade Unit PlanDokumen19 halamanA Seventh Grade Unit Plandbradl22Belum ada peringkat
- How To Self-Assess For Maximum Impact Within An OrganizationDokumen21 halamanHow To Self-Assess For Maximum Impact Within An OrganizationOthniel EmejeBelum ada peringkat
- Morpho-Syntax IntroductionDokumen5 halamanMorpho-Syntax IntroductionMelaniaBelum ada peringkat
- Data Science - Machine LearningDokumen3 halamanData Science - Machine Learningfaheem ahmedBelum ada peringkat
- A Translanguaging Pedagogy For Writing A CUNY-NYSIEB Guide For Educators ArquivoDokumen119 halamanA Translanguaging Pedagogy For Writing A CUNY-NYSIEB Guide For Educators ArquivoMariana HungriaBelum ada peringkat
- Unit 2 - Today'S Topic Is : English Public Speaking & Presentation (Advanced) Week 5 Professor HayashiDokumen15 halamanUnit 2 - Today'S Topic Is : English Public Speaking & Presentation (Advanced) Week 5 Professor HayashiAmy HayashiBelum ada peringkat
- PerdevDokumen10 halamanPerdevdarlene martinBelum ada peringkat
- What Makes A Helpful Online Review? A Study of Customer Reviews OnDokumen17 halamanWhat Makes A Helpful Online Review? A Study of Customer Reviews OnBreak HabitBelum ada peringkat
- Assessment Our Finding ShowDokumen3 halamanAssessment Our Finding ShowDrouai Wafa100% (1)
- Basic & Architectural DesignDokumen20 halamanBasic & Architectural Designkeerthikakandasamy100% (1)
- Iect Motivation LetterDokumen1 halamanIect Motivation LetteranshBelum ada peringkat
- KD21C Model Answer KeyDokumen2 halamanKD21C Model Answer KeymadhuBelum ada peringkat
- Introduction To Humanities: Lori-Beth LarsenDokumen70 halamanIntroduction To Humanities: Lori-Beth LarsenCharmaine JanorasBelum ada peringkat