Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Pi Is 0889540610008954Dokumen10 halamanPi Is 0889540610008954Roberto OlaveBelum ada peringkat
- Pi Is 0889540610008954Dokumen10 halamanPi Is 0889540610008954Roberto OlaveBelum ada peringkat
- Molar ProtactionDokumen9 halamanMolar ProtactionRoberto OlaveBelum ada peringkat
- 1986 Dermaut Et Al. Experimental Determination of The Center of Resistance of The Upper FirstDokumen8 halaman1986 Dermaut Et Al. Experimental Determination of The Center of Resistance of The Upper Firstosama-alaliBelum ada peringkat
- Pi Is 0889540610008954Dokumen10 halamanPi Is 0889540610008954Roberto OlaveBelum ada peringkat
- Desarrollo Oclusión - Baume IDokumen7 halamanDesarrollo Oclusión - Baume IRoberto OlaveBelum ada peringkat
- Bionator IIIDokumen5 halamanBionator IIIRoberto OlaveBelum ada peringkat
- Center of ResistenceDokumen15 halamanCenter of ResistencemutansBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- SIGNS IN OTORHINOLARYNGOLOGYDokumen5 halamanSIGNS IN OTORHINOLARYNGOLOGYVetrivel TamizhBelum ada peringkat
- 24 - Pharyngeal Arches and Its DerivativesDokumen32 halaman24 - Pharyngeal Arches and Its DerivativesDr.B.B.GosaiBelum ada peringkat
- KeaBalo Highlight Ombre Lace Front Wigs Human Hair Pre Plucked With Baby Hair 13x4 Body Wave Frontal Wigs Human HaiDokumen1 halamanKeaBalo Highlight Ombre Lace Front Wigs Human Hair Pre Plucked With Baby Hair 13x4 Body Wave Frontal Wigs Human HaiCelina BurnsBelum ada peringkat
- Anatomy and Clinical Significance of Denture Bearing AreasDokumen60 halamanAnatomy and Clinical Significance of Denture Bearing AreasheycoolalexBelum ada peringkat
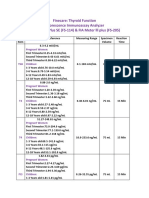
- Thyroid FunctionDokumen2 halamanThyroid FunctionSm Bikash Kumar MohonBelum ada peringkat
- Treatment Planning of ImplantsDokumen10 halamanTreatment Planning of ImplantsRussia Al ShboulBelum ada peringkat
- The TracheaDokumen16 halamanThe TracheaMatende husseinBelum ada peringkat
- Axial Skeleton ScriptDokumen4 halamanAxial Skeleton ScriptMichaelVincentLimBelum ada peringkat
- Thyroid Disorders in Bangladesh-Past, Present and Future: EditorialDokumen2 halamanThyroid Disorders in Bangladesh-Past, Present and Future: Editorialmitu lead01Belum ada peringkat
- Cervical Plexus: Anatomy Presentation Submitted To: Ma'Am Nain Tara DPT 1 Proff (Morning)Dokumen22 halamanCervical Plexus: Anatomy Presentation Submitted To: Ma'Am Nain Tara DPT 1 Proff (Morning)Hira Waseem100% (1)
- OC StudentDokumen2 halamanOC Studentszekeres annamariBelum ada peringkat
- Messy TwistDokumen17 halamanMessy TwistPrincess MoonlihgtBelum ada peringkat
- Oralna Hirurgija Spremanje UsmenogDokumen7 halamanOralna Hirurgija Spremanje UsmenogHarunKarovićBelum ada peringkat
- ANATOMY ORAL CAVITY and TONGUE JelDokumen54 halamanANATOMY ORAL CAVITY and TONGUE JelCoy EnBelum ada peringkat
- Orthodontic AssessmentDokumen30 halamanOrthodontic Assessmentmentacity10100% (2)
- Lecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesDokumen73 halamanLecture Outline: See Separate Powerpoint Slides For All Figures and Tables Pre-Inserted Into Powerpoint Without NotesAngelika DomondonBelum ada peringkat
- Prostodontics Antomical & Physiological ConsiderationsDokumen10 halamanProstodontics Antomical & Physiological ConsiderationsfitsumBelum ada peringkat
- ENT MCQs (Girls 1428-29)Dokumen7 halamanENT MCQs (Girls 1428-29)Sheikha100% (9)
- MAXEN WELLNESS JOINING PACKSDokumen8 halamanMAXEN WELLNESS JOINING PACKSAnkur SrivastavaBelum ada peringkat
- Oral CavityDokumen20 halamanOral CavityadileidalaaBelum ada peringkat
- Practice Test Questions Downloaded From FILIPINO NURSES CENTRALDokumen4 halamanPractice Test Questions Downloaded From FILIPINO NURSES CENTRALFilipino Nurses CentralBelum ada peringkat
- Lewis: Medical-Surgical Nursing, 8 Edition: Chapter 21: Nursing Assessment: Visual and Auditory Systems Test BankDokumen8 halamanLewis: Medical-Surgical Nursing, 8 Edition: Chapter 21: Nursing Assessment: Visual and Auditory Systems Test BankMonicaBelum ada peringkat
- Venous Blood Sinuses Guide: Anatomy, Drainage & Clinical NotesDokumen15 halamanVenous Blood Sinuses Guide: Anatomy, Drainage & Clinical NotesJennifer RodriguezBelum ada peringkat
- Errors Associated With Digital Preview of Computer-Engineered Complete Dentures and Guidelines For Reducing Them: A Technique ArticleDokumen11 halamanErrors Associated With Digital Preview of Computer-Engineered Complete Dentures and Guidelines For Reducing Them: A Technique ArticletovarichBelum ada peringkat
- Phonology DefinedDokumen16 halamanPhonology DefinedFhanyBelum ada peringkat
- Vijay Kautilya DDokumen121 halamanVijay Kautilya DNashBelum ada peringkat
- Endemic and Sporadic GoiterDokumen13 halamanEndemic and Sporadic GoiterBtwo SoelBelum ada peringkat
- Atlas of Large Animal SurgeryDokumen147 halamanAtlas of Large Animal SurgeryJohn Cadenillas RumayBelum ada peringkat
- Anatomi Kepala Dan Leher: Oleh: Abdullah Putra Perdana Ppds Ilmu Bedah FK Ulm 2017Dokumen32 halamanAnatomi Kepala Dan Leher: Oleh: Abdullah Putra Perdana Ppds Ilmu Bedah FK Ulm 2017drhendyjuniorBelum ada peringkat