Anda mungkin juga menyukai
- Brain CureDokumen157 halamanBrain CureJosh BillBelum ada peringkat
- Home Remedies For Vertigo - DizzinessDokumen11 halamanHome Remedies For Vertigo - DizzinesstslaitraBelum ada peringkat
- The Endocrine Glands ExplainedDokumen13 halamanThe Endocrine Glands ExplainedEd CrownBelum ada peringkat
- What is Demyelination? Understanding the Causes, Symptoms and TreatmentDokumen7 halamanWhat is Demyelination? Understanding the Causes, Symptoms and TreatmentGeorge ForțuBelum ada peringkat
- The Three Personality Types of AyurvedaDokumen11 halamanThe Three Personality Types of AyurvedaIrem YitmenBelum ada peringkat
- ElectroHomopathicMedicine 10016840Dokumen371 halamanElectroHomopathicMedicine 10016840colpmdasBelum ada peringkat
- GeneticsDokumen50 halamanGeneticsanneBelum ada peringkat
- Black SalveDokumen3 halamanBlack SalveGolden SunriseBelum ada peringkat
- Hemolytic Anemia - Evaluation and Differential DiagnosisDokumen8 halamanHemolytic Anemia - Evaluation and Differential Diagnosiscarolinapolotorres100% (1)
- HISTORY OF MATHEMATICSDokumen5 halamanHISTORY OF MATHEMATICSAsley Kate BienBelum ada peringkat
- Blood Type PersonalitiesDokumen8 halamanBlood Type Personalitiesapi-411384401Belum ada peringkat
- GABA Receptors and The Immune System-012012Dokumen23 halamanGABA Receptors and The Immune System-012012idjacobsBelum ada peringkat
- Palmistry Signs: Meanings of the Star, Cross, Triangle, Circle and DotDokumen4 halamanPalmistry Signs: Meanings of the Star, Cross, Triangle, Circle and Dotzaim techBelum ada peringkat
- The Rational Basis of "Nature Cure" PDFDokumen4 halamanThe Rational Basis of "Nature Cure" PDFkrishna2205Belum ada peringkat
- A History of Pharmaceutical CompoundingDokumen6 halamanA History of Pharmaceutical CompoundingAnastasius HendrianBelum ada peringkat
- Unit 5: Healing SystemDokumen24 halamanUnit 5: Healing SystemSushmita BudhathokiBelum ada peringkat
- Benha University Hospital fertility staging systemDokumen42 halamanBenha University Hospital fertility staging systemmadmax500Belum ada peringkat
- Biochemistry Research PaperDokumen10 halamanBiochemistry Research Paperapi-512419266Belum ada peringkat
- Alexander BainDokumen6 halamanAlexander BainNur HaBelum ada peringkat
- DR Debra Betts.: PHD Lac Illustrations Compiled by Tina YoungDokumen14 halamanDR Debra Betts.: PHD Lac Illustrations Compiled by Tina YoungSamo SanjaBelum ada peringkat
- Heart and Circulation Natural Authority by Rosina Sonnenschmidt Reading ExtractDokumen12 halamanHeart and Circulation Natural Authority by Rosina Sonnenschmidt Reading ExtractSohail LatifBelum ada peringkat
- Germany Homeopathic Medicines ListDokumen66 halamanGermany Homeopathic Medicines Listar hijaziBelum ada peringkat
- US Rare Earth Minerals, Inc. - EXCELERITE Technical ReportDokumen12 halamanUS Rare Earth Minerals, Inc. - EXCELERITE Technical ReportUSREMBelum ada peringkat
- MTOR Is A Key Modulator of Ageing and Age-Related Disease: Nature January 2013Dokumen9 halamanMTOR Is A Key Modulator of Ageing and Age-Related Disease: Nature January 2013SBBelum ada peringkat
- Respiration WorksheetDokumen5 halamanRespiration WorksheetFendy Hamid67% (6)
- Practice Essentials: Essential Update: Chemotherapy Following Radiation May Improve Survival in Low-Grade GliomasDokumen19 halamanPractice Essentials: Essential Update: Chemotherapy Following Radiation May Improve Survival in Low-Grade GliomasFika Khulma SofiaBelum ada peringkat
- DNA Waves and WaterDokumen10 halamanDNA Waves and WatereioBelum ada peringkat
- Canine Hypoadrenocorticism Pathogenesis and Clinical FeaturesDokumen9 halamanCanine Hypoadrenocorticism Pathogenesis and Clinical FeaturesAna Clara SevasteBelum ada peringkat
- Clinical Examination - A Systematic Guide To Physical Diagnosis, 7th Ed (PDF) (Tahir99) VRG - pdf1259358830Dokumen55 halamanClinical Examination - A Systematic Guide To Physical Diagnosis, 7th Ed (PDF) (Tahir99) VRG - pdf1259358830Anonymous 5CdXo6j0nBelum ada peringkat
- Lancet Article PDFDokumen5 halamanLancet Article PDFBrandy GarciaBelum ada peringkat
- ملخص قطرة مطر 37 سؤالDokumen6 halamanملخص قطرة مطر 37 سؤالShatha MustafaBelum ada peringkat
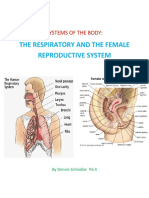
- Systems of The BodyDokumen10 halamanSystems of The BodyKatrina SchindlarBelum ada peringkat
- Chromosomes and ChromatinDokumen52 halamanChromosomes and ChromatinMuhammad Haroon100% (1)
- Suzie BiofeedbackSDCRIDokumen3 halamanSuzie BiofeedbackSDCRIocortezlariosBelum ada peringkat
- Glossary Fundamentals in NursingDokumen32 halamanGlossary Fundamentals in NursingSJay Herrero100% (3)
- Case Study - Seizuring DogDokumen8 halamanCase Study - Seizuring Dogapi-301746262Belum ada peringkat
- Bahasa Inggeris Paper 1 f1Dokumen9 halamanBahasa Inggeris Paper 1 f1Norasidah AgmanBelum ada peringkat
- The Spectrum of Mitochondrial Disease Ep-3-10Dokumen8 halamanThe Spectrum of Mitochondrial Disease Ep-3-10F4AR100% (1)
- Dr. Stevens's System of Medical ElectricityDokumen20 halamanDr. Stevens's System of Medical Electricityaryaa2020Belum ada peringkat
- A Test in Context - D-DimerDokumen10 halamanA Test in Context - D-DimerRoberto López MataBelum ada peringkat
- Small Molecule Activators of Sirtuins Extend Saccharomyces Cerevisiae LifespanDokumen5 halamanSmall Molecule Activators of Sirtuins Extend Saccharomyces Cerevisiae LifespanMiguel Angel Salazar SánchezBelum ada peringkat
- Article - Telomerase Reverses Ageing ProcessDokumen3 halamanArticle - Telomerase Reverses Ageing Processapi-240998846Belum ada peringkat
- MicroReview-Small Molecules That Regulate Lifespan-Evidence For XenohormesisDokumen7 halamanMicroReview-Small Molecules That Regulate Lifespan-Evidence For Xenohormesismarijana_zBelum ada peringkat
- This Is The Ultimate Cure For All Vision Problems - Recipe - HealthycaregroupDokumen4 halamanThis Is The Ultimate Cure For All Vision Problems - Recipe - Healthycaregroupanubhavg82Belum ada peringkat
- Resveratrol Improves Health and Survival of Mice On A High-Calorie DietDokumen6 halamanResveratrol Improves Health and Survival of Mice On A High-Calorie Dietapi-119817014Belum ada peringkat
- 10 Blood Tests For Vegans & VegetariansDokumen3 halaman10 Blood Tests For Vegans & VegetariansWeb WorldBelum ada peringkat
- The Meaning of NamesDokumen7 halamanThe Meaning of NamesJo LinfordBelum ada peringkat
- Telomere Biology & CancerDokumen9 halamanTelomere Biology & CancerMelissa WilderBelum ada peringkat
- Adrenal Cortex and Medulla - The Clinical ContextDokumen10 halamanAdrenal Cortex and Medulla - The Clinical ContextbluesaltBelum ada peringkat
- NAD+ Replenishment Improves Lifespan and Healthspan in Ataxia Telangiectasia Models Via Mitophagy and DNA RepairDokumen47 halamanNAD+ Replenishment Improves Lifespan and Healthspan in Ataxia Telangiectasia Models Via Mitophagy and DNA Repairender000100% (1)
- The Brain and BotanicalsDokumen28 halamanThe Brain and BotanicalsbonziebodyBelum ada peringkat
- Telomere PDFDokumen2 halamanTelomere PDFsoumita100% (1)
- New Text Document1235Dokumen8 halamanNew Text Document1235Patrice Pratt100% (1)
- TELOMEREDokumen17 halamanTELOMEREPRATAPBelum ada peringkat
- Posterior Pituitary Gland Presentation - paraDokumen40 halamanPosterior Pituitary Gland Presentation - parahamidBelum ada peringkat
- Biology of DepressionDokumen5 halamanBiology of DepressionScience RespondsBelum ada peringkat
- List of Genetically Transmitted DiseasesDokumen3 halamanList of Genetically Transmitted DiseasesKara Mae Pagcanlungan Sugui100% (1)
- Safety Issues Affecting Herbs - Pyrrolizidine AlkaloidsDokumen11 halamanSafety Issues Affecting Herbs - Pyrrolizidine AlkaloidsleyendosinpararBelum ada peringkat
- NIACINDokumen4 halamanNIACINJustin Paul ChanBelum ada peringkat
- FolateDokumen18 halamanFolateNauman ShakirBelum ada peringkat
- SporotrichosisDokumen15 halamanSporotrichosisDexel Putra SimbolonBelum ada peringkat
- Pendular Diagnosis - From Dowsing To Diagnostic MethodologyDokumen7 halamanPendular Diagnosis - From Dowsing To Diagnostic MethodologyVijay MuthekarBelum ada peringkat
- Group Assignment 2 - Analysis On Marketing EnvironmentDokumen21 halamanGroup Assignment 2 - Analysis On Marketing EnvironmentAisyah AfiqahBelum ada peringkat
- Deep Fungal InfectionsDokumen33 halamanDeep Fungal Infectionstummalapalli venkateswara raoBelum ada peringkat
- Doctrines of Demons by Tricia Tillin Birthpangs - OrgDokumen217 halamanDoctrines of Demons by Tricia Tillin Birthpangs - OrgTricia Tillin0% (1)
- Micro Endocrine OrgansDokumen8 halamanMicro Endocrine OrgansMonica100% (1)
- 3553 FullDokumen10 halaman3553 FullFika Khulma SofiaBelum ada peringkat
- Hal 1-4Dokumen8 halamanHal 1-4Fika Khulma SofiaBelum ada peringkat
- 3553 FullDokumen10 halaman3553 FullFika Khulma SofiaBelum ada peringkat
- Hal 58-62Dokumen9 halamanHal 58-62Fika Khulma SofiaBelum ada peringkat
- Dapusimun 1Dokumen7 halamanDapusimun 1Fika Khulma SofiaBelum ada peringkat
- Psikimetab10 2012Dokumen2 halamanPsikimetab10 2012Fika Khulma SofiaBelum ada peringkat
- Tambahan ImunologiDokumen5 halamanTambahan ImunologiFika Khulma SofiaBelum ada peringkat
- Case Headache On PregnancyDokumen5 halamanCase Headache On PregnancyFika Khulma SofiaBelum ada peringkat
- Costa MDokumen1 halamanCosta MFika Khulma SofiaBelum ada peringkat
- Morning Report Februari 2016: A 36-Year-Old-Man With Moderate Acute Asthma DD Acis DD CopdDokumen14 halamanMorning Report Februari 2016: A 36-Year-Old-Man With Moderate Acute Asthma DD Acis DD CopdFika Khulma SofiaBelum ada peringkat
- Abstrak DR SariDokumen2 halamanAbstrak DR SariFika Khulma SofiaBelum ada peringkat
- InTech - Mechanisms in Erectile Function and Dysfunction An OverviewDokumen21 halamanInTech - Mechanisms in Erectile Function and Dysfunction An OverviewFika Khulma SofiaBelum ada peringkat
- Incidence of Venous Air Embolism During Craniectomy For Craniosynostosis RepairDokumen4 halamanIncidence of Venous Air Embolism During Craniectomy For Craniosynostosis RepairFika Khulma SofiaBelum ada peringkat
- Jurnal Vian 4Dokumen12 halamanJurnal Vian 4Fika Khulma SofiaBelum ada peringkat
- Venembol 2Dokumen19 halamanVenembol 2Fika Khulma SofiaBelum ada peringkat
- The Evolving Role of Hysterectomy in Gestational Trophoblastic Neoplasia at The New England Trophoblastic Disease CenterDokumen2 halamanThe Evolving Role of Hysterectomy in Gestational Trophoblastic Neoplasia at The New England Trophoblastic Disease CenterFika Khulma SofiaBelum ada peringkat
- Cardioplegia in Pediatric Cardiac Surgery: Do We Believe in Magic?Dokumen12 halamanCardioplegia in Pediatric Cardiac Surgery: Do We Believe in Magic?Fika Khulma SofiaBelum ada peringkat
- Venous Air Embolism During Anterior Lumbar Surgery: Case ReportDokumen3 halamanVenous Air Embolism During Anterior Lumbar Surgery: Case ReportFika Khulma SofiaBelum ada peringkat
- CRD 9Dokumen12 halamanCRD 9Fika Khulma SofiaBelum ada peringkat
- CRD 1Dokumen2 halamanCRD 1Fika Khulma SofiaBelum ada peringkat
- CRD 6Dokumen7 halamanCRD 6Fika Khulma SofiaBelum ada peringkat
- Time Course of Elevations in Plasma Olprinone Concentration During Pediatric Cardiac SurgeryDokumen4 halamanTime Course of Elevations in Plasma Olprinone Concentration During Pediatric Cardiac SurgeryFika Khulma SofiaBelum ada peringkat
- 2 Myocardial Protection in Pediatric Cardiac SurgeryDokumen6 halaman2 Myocardial Protection in Pediatric Cardiac SurgeryFika Khulma Sofia100% (1)
- CRD 8Dokumen7 halamanCRD 8Fika Khulma SofiaBelum ada peringkat
- Br. J. Anaesth.-2012-S Rensen-682-9Dokumen8 halamanBr. J. Anaesth.-2012-S Rensen-682-9Fika Khulma SofiaBelum ada peringkat
- Single Dose Inamrinone in Terminal Warm Cardioplegia in On-Pump Coronary Artery Bypass PatientsDokumen5 halamanSingle Dose Inamrinone in Terminal Warm Cardioplegia in On-Pump Coronary Artery Bypass PatientsFika Khulma SofiaBelum ada peringkat
- Jurnal Vian 4Dokumen12 halamanJurnal Vian 4Fika Khulma SofiaBelum ada peringkat
- Spinal 6Dokumen3 halamanSpinal 6Fika Khulma SofiaBelum ada peringkat
- FAQ On Blood DonationDokumen2 halamanFAQ On Blood DonationAnilBelum ada peringkat
- Daratumumab in Life-Threatening Autoimmune Hemolytic Anemia Following Hematopoietic Stem Cell TransplantationDokumen4 halamanDaratumumab in Life-Threatening Autoimmune Hemolytic Anemia Following Hematopoietic Stem Cell Transplantationmohana reddyBelum ada peringkat
- System of The Body Pre Test M2Dokumen7 halamanSystem of The Body Pre Test M2joesmithmedina1988Belum ada peringkat
- Protocol TPEDokumen19 halamanProtocol TPEPatricia TamasBelum ada peringkat
- Pengaruh Autogenik3Dokumen5 halamanPengaruh Autogenik3Ruslan MuhammadBelum ada peringkat
- Blood System 5 PDFDokumen10 halamanBlood System 5 PDFSardar jiBelum ada peringkat
- Detect and ID Unexpected AntibodiesDokumen10 halamanDetect and ID Unexpected AntibodiesWayne VillalunaBelum ada peringkat
- CCHD ScreeningDokumen3 halamanCCHD ScreeningAhmad ThotuchingBelum ada peringkat
- Transportation in Plants and Animals Ncert and Extra QuestionsDokumen6 halamanTransportation in Plants and Animals Ncert and Extra QuestionsNaitik MeenaBelum ada peringkat
- PranithaDokumen15 halamanPranithaKumar VijayBelum ada peringkat
- Autoimmune Hemolytic Anemia Diagnosis and Differential DiagnosisDokumen10 halamanAutoimmune Hemolytic Anemia Diagnosis and Differential DiagnosisMARCO MONTES REYESBelum ada peringkat
- Clinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDokumen4 halamanClinico-Aetiological Profile of Pancytopenia in Paediatric PracticeDesi AdiyatiBelum ada peringkat
- The An Them We Have The Second One That Is The: Causes of AnemiaDokumen6 halamanThe An Them We Have The Second One That Is The: Causes of AnemiakimberlynBelum ada peringkat
- Drug Study - HemostanDokumen2 halamanDrug Study - Hemostangoody1286Belum ada peringkat
- GR10 M01 Lesson-1-PowerpointDokumen103 halamanGR10 M01 Lesson-1-PowerpointRv RamosBelum ada peringkat
- Anemia Overview: The Third Hospital of Sun Yat-Sen UniversityDokumen77 halamanAnemia Overview: The Third Hospital of Sun Yat-Sen UniversityMazlina MaidinBelum ada peringkat
- Gaksung Wave (Eng)Dokumen6 halamanGaksung Wave (Eng)Gaksung GlobalBelum ada peringkat
- ABC Blood Letting InvitationDokumen2 halamanABC Blood Letting InvitationKeeshia Tenise BadillesBelum ada peringkat
- Paragraph Completion 4Dokumen8 halamanParagraph Completion 4SuziBelum ada peringkat
- Sir Ganga Ram Hospital Schedule of Charges 2017-18Dokumen315 halamanSir Ganga Ram Hospital Schedule of Charges 2017-18Amit Kumar GuptaBelum ada peringkat
- 12 Step To Accurately Measuring Blood PressureDokumen4 halaman12 Step To Accurately Measuring Blood PressureJonelle GreeneBelum ada peringkat
- Chromatogram Interpretation Aids: HLC-723G11 SS-Thalassaemia Analysis ModeDokumen2 halamanChromatogram Interpretation Aids: HLC-723G11 SS-Thalassaemia Analysis ModeAlaa' MusafferBelum ada peringkat
- The Respirator Y System: Mungcal, Dharlynette RTRPDokumen158 halamanThe Respirator Y System: Mungcal, Dharlynette RTRPDharlyn MungcalBelum ada peringkat
- Biology 8461/1H: Mark SchemeDokumen27 halamanBiology 8461/1H: Mark SchemeMohamad HabbalBelum ada peringkat