IOSR Journal of Dental and Medical Sciences (IOSR-JDMS)
e-ISSN: 2279-0853, p-ISSN: 2279-0861.Volume 14, Issue 10 Ver.VII (Oct. 2015), PP 126-131
www.iosrjournals.org
Comparison of Dexmedetomidine, Esmolol and Sodium
Nitroprusside for Hypotensive Anaesthesia in Functional
Endoscopic Sinus Surgery
Mushtaq Ahmad Rather, Farhana Bashir and Saba Ahad
1,2
Department of anesthesiology and critical care GMC Srinagar, 190006.
Abstract:
Background: This study has been designed to compare the controlled hypotensive effects of Dexmedetomidine
(DEX), Sodium Nitroprusside (SNP) and Esmolol (ESM) during functional endoscopic sinus surgery (FESS).
Method: In a prospective, double-blind study; we randomized 45 (15 in each group) ASA physical status I and
II patients in the age group 18-60 years scheduled for FESS to receive either DEX (group 1) loading dose of
1g/kg 10 mins before induction of anaesthesia followed by infusion at the rate of 0.4-0.8g/kg/hr during
maintenance of anaesthesia or SNP (group 2) 0.5-10g/kg/min infusion after induction of anaesthesia or ESM
group loading dose of 1mg/kg infused over 1 min followed by maintenance rate of 0.4-0.8mg/kg/hr. All the
infusion rates were titrated to maintain the mean arterial pressure (MAP) between 60-70 mmHg so as to
minimise the intraoperative bleeding.
Results: DEX resulted in significant reduction in MAP, heart rate, better intraoperative field conditions and the
time required for first rescue analgesia was longer. ESM and SNP were associated with significantly shorter
extubation and recovery time than DEX. SNP provided a relatively poor surgical condition than observed in
ESM/DEX.
Conclusion: DEX is relatively safe and effective agent followed by ESM than SNP for controlled hypotension in
patients undergoing FESS.
Key-words: Anaesthesia,Dexmedetomidine, Esmolol, Sodium Nitroprusside, controlled hypotension,
Functional endoscopic sinus surgery
I.
Introduction
FESS is most commonly performed for inflammatory and infectious sinus diseases like chronic
sinusitis, nasal polyposis,sinus mucoceles,antrochoanal polyps etc.Typically FESS is reserved for patients with
documented rhinosinusitis in whom appropriate medical treatment has failed[1].The major complications of
FESS like optic nerve damage ,meningitis and damage to duraresult from impaired visibility due to excessive
bleeding in the surgical field[2].Deliberate hypotension is a common technique to decrease blood loss and
improve the operative field visualisation during different types of surgical procedures[3].Deliberate
hypotension involves reducing arterial blood pressure 40-50% below its normal range or reducing mean
arterial blood pressure to 60mmhg intentionally and recoverably and maintaining it at this level throughout
the operative process[4].
Various agents like sodium nitroprusside,esmolol,nitroglycerine,dexmedetomidine etc. have been
used for deliberate hypotension in various surgeries to control bleeding.Present study has been conducted to
compare theefficacy of dexmedetomidine,esmolol and sodium nitroprusside for inducing hypotension in FESS.
II.
Material And Method
After seeking approval from institutional ethical committee, 45 ASA I and II patients scheduled for
FESS were enrolled in the study. Participants were in the age group 18 to 60years. Patients less than 18 years,
those preferring local anaesthesia, those who were on cardiovascularly active drugs or drugs influencing blood
coagulation (Warfarin, heparin, enoxaparin, or aspirin) were excluded from the study. Patients were randomly
distributed in three groups DEX (group 1), SNP (group 2) and ESM (group 3); 15 patients in each group.
All the patients received premedication according to the hospital protocol; midazolam 0.5-1mg
intravenously followed by fentanyl 0.5-2g/kg intravenously (IV) 2-3 mins before induction of anaesthesia
which was done by 2mg/kg propofol IV and rocuronium 0.6-1.2mg/kg IV was used to facilitate tracheal
intubation with oral cuffed tracheal tube. Anaesthesia was maintained by 50% nitrous oxide with oxygen and
1% isoflurane. IV fluid lactated Ringer was used for hydrating the patients at approximately 3ml/kg/hr. Patients
were placed in 5 reverse trendelenbergs position to improve venous drainage. All patients received paracetamol
15-20mg/kg infusion IV over 20mins as an additional analgesic intraoperatively.
DOI: 10.9790/0853-14107126131
www.iosrjournals.org
126 | Page
Comparison of Dexmedetomidine, Esmolol and Sodium Nitroprusside for Hypotensive Anaesthesia...
Monitoring included MAP using 20G arterial cannula for direct blood pressure measurement, heart rate
with electrocardiogram (ECG), and to assess the amount of bleeding in operative field we used 6 point category
scale:
0 no bleeding;
1 slight bleeding- no suctioning of blood required;
2 slight bleeding- occasional suctioning required, surgical field not threatened;
3 slight bleeding- frequent suctioning required, bleeding threatens surgical field a few seconds after
suction is removed;
4 moderate bleeding- frequent suctioning required, bleeding threatens surgical field directly after
suction is removed;
5 severe bleeding- constant suctioning required, bleeding appears faster than can be removed by
suction, surgical field severely threatened and surgery not possible.
Above monitoring parameters were in addition to the other routine parameters like oxygen saturation
(SPO2) and end tidal CO2 (ETCO2).
Group 1 received a loading dose of DEX 1g/kg 10 mins before induction of anaesthesia followed by
infusion at the rate of 0.4-0.8g/kg/hr during maintenance of anaesthesia and titrated till the desired MAP of 6070mmHg was achieved.
Group 2 received 0.5-10g/kg/min infusion of SNP after induction of anaesthesia and titrated
accordingly to achieve target MAP.
Group 3 received loading dose of 1mg/kg of ESM infused over 1 min followed by maintenance rate of
0.4-0.8mg/kg/hr and titrated till target MAP achieved.
MAP and heart rate were measured and monitored by the anaesthetist who was blinded to the use of
hypotensive drug and surgical field bleeding was measured by the surgeon by the 6 point category scale. The
surgeon was blinded to the use of hypotensive agent as well as to the hemodynamic variables.
In all the 3 groups signs of inadequate anaesthesia (eg. increase in arterial pressuregreater than the
targeted MAP) or somatic responses (eg. movement, tearing, orsweating) were treated with additional fentanyl.
Infusion of the study drugs was stopped 5 minutes before the anticipated end of surgery and isoflurane
was stopped after skin closure. After the surgery was finished, each patient received neostigmine (50-70g/kg)
with atropine (20g/kg). Extubation time along with time to recovery was recorded in each group using Aldrete
score. Aldrete score 9 on a scale of 010. Each variable was scored on a 3-point scaleconsciousness[2 =
fully awake; 1 = able to be roused on calling; 0 = not responding], activity [ableto move voluntarily or on
command: 2 = 4 extremities; 1 = 2 extremities; 0 = 0 extremities],respiration [2 = able to breathe deeply and
cough freely; 1 = dyspnoea, shallowor limited breathing; 0 = apnoeic], circulation [2 = blood pressure (BP)
}<20 mmof Preanaesthestic level; 1 = BP }2050 mm of Preanaesthestic level; 0 = BP }>50 mmof
Preanaesthestic level], and SpO2 [2 = >92% on room air; 1 = needs oxygen inhalationto maintain SpO2 >90%;
0 = SpO2 <90% even with oxygen supplementation]with a maximum achievable score of 10).
Post recovery patients were shifted to the post anaesthesia care unit and were monitored for any
adverse effect if any like intraoperative hypotension [MAP<60 mm Hg], bradycardia [HR <50 beats/min],
postoperativefentanyl consumption, and postoperative nausea and vomiting. The sedation score was measured
using the following scale at 15, 30, and 60 minutes after tracheal extubation: 1 = anxious,agitated, or restless; 2
= cooperative, oriented, and tranquil; 3 = responsive to commands;4 = asleep, but with brisk response to light,
glabellar tap, or loud auditorystimulus; 5 = asleep, sluggish response to glabellar tap or auditory stimulus; and 6
=asleep, no response.
III.
Results
Forty five patients were enrolled in this study undergoing a FESS (15 each in the DEX, SNP and ESM
group). All patients were able to complete the entire study and their data were included in the final analysis. The
demographic data, duration of surgery, intraoperative blood loss, and duration of anesthesia were compared
between the two groups. All the groups were comparable in terms of age, sex, weight, duration of surgery, and
duration of anesthesia (Table 1).
Table 1:- Demographic and operative data.
Parameter
Age(yrs)
Male : Female
Weight(kg)
ASA I: ASA II
Duration of Anaesthesia(min)
Duration of surgery(min)
Group 1(DEX)
40.1211.9
9:6
64.589.20
8:7
91.1210.03
80.1211.50
DOI: 10.9790/0853-14107126131
Group 2(SNP)
42.1210.07
8:7
63.128.92
9:6
94.089.55
83.089.45
www.iosrjournals.org
Group 3(ESM)
39.1212.77
7:8
608.95
7:8
93.038.65
81.0310.45
P-Value
0.190
0.980
0.582
0.791
0.910
0.139
127 | Page
Comparison of Dexmedetomidine, Esmolol and Sodium Nitroprusside for Hypotensive Anaesthesia...
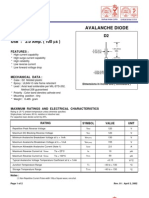
Blood loss was significantly less in the DEX group than in the SNP and ESM group. The changes in
MAP between the three groups were statistically insignificant at preoperative, 15 min, 30min,45min and 60 min
intraoperative, and after recovery, but were significantly lower in the DEX group than the SNP, ESM group at
post-induction, 5 min and 10 min after stopping of hypotensive agents (Table 2 and Fig. 1).
Table 2:- Mean arterial pressure values (mmHg) in the dexmedetomidine (DEX), sodium Nitroprusside
(SNP) and esmolol (ESM) groups at different times
preoperative
Group
1(DEX)
91.59.3
Group
2(SNP)
92.89.5
Group
3(ESM)
90.79.2
post induction
71.36.7
82.16.5
79.96.7
15 min intra operative
65.26.4
67.85.9
63.76.2
30 min intraoperative
60.45.8
63.76.0
62.15.7
45 min intra operative
61.25.5
62.85.5
62.96.5
60 min intraoperative
60.44.5
64.44.5
63.75.3
5 min after stopping hypotensive agent
63.56.4
80.75.3
79.56.5
10 min after stopping hypotensive agent
71 9.4
87.98.9
86.39.0
after recovery
85.48.5
93.47.9
92.58.3
100
90
p-value
1 vs 2 Ns
1 vs 3 Ns
2 vs 3 Ns
1 vs 2 S
1 vs 3 S
2 vs 3 S
1 vs 2 Ns
1 vs 3 Ns
2 vs 3 Ns
1 vs 2 Ns
1 vs 3 Ns
2 vs 3 Ns
1 vs 2 Ns
1 vs 3 Ns
2 vs 3 Ns
1 vs 2 Ns
1 vs 3 Ns
2 vs 3 Ns
1 vs 2 S
1 vs 3 S
2 vs 3 S
1 vs 2 S
1 vs 3 S
2 vs 3 S
1 vs 2 Ns
1 vs 3 Ns
2 vs 3 Ns
Figure : Showing Mean Arterial Pressure (MAP) at different times
80
70
60
Group DEX
50
Group SNP
40
Group ESM
The changes in HR between the two groups werestatistically insignificant at preoperativeand after
recover, but weresignificantly lower in the DEX and ESM group than theSNP group at post induction, 15 min
intra operative,30 min intraoperative, 45 min intra operative, 60 min intraoperative. However the heart rate
increased significantly in ESM group than in DEX groupat 5 and 15 min after stopping of hypotensive agents
(Table 3and Fig. 2).
There were no episodes of severe hypotension (MAP of 60mmHg) or severe bradycardia (HRof
50beats/min) duringinfusion of the hypotensive agents in both groups.
DOI: 10.9790/0853-14107126131
www.iosrjournals.org
128 | Page
Comparison of Dexmedetomidine, Esmolol and Sodium Nitroprusside for Hypotensive Anaesthesia...
Table 2:- Heart rate values (BPM) in the dexmedetomidine (DEX), odium Nitroprusside (SNP) and
esmolol (ESM) groups at different times
Group
1(DEX)
80.38.5
Group
2(SNP)
83.48.6
Group
3(ESM)
81.68.9
post induction
63.27.4
70.27.9
66.68.0
15 min intra operative
60.75.4
89.45.9
62.26.0
30 min intraoperative
59.76.6
88.15.9
60.06.0
45 min intra operative
61.74.5
90.54.7
63.25.0
60 min intraoperative
62.85.4
92.94.5
64.75.5
5 min after stopping hypotensive agent
63.24.8
79.65.7
76.36.8
10 min after stopping hypotensive agent
72.68.5
78.28.1
80.88.9
after recovery
73.38.8
80.99.0
83.67.9
preoperative
p-value
1 vs 2 Ns
1 vs 3 Ns
2 vs 3 Ns
1 vs 2 S
1 vs 3 Ns
2 vs 3 S
1 vs 2 S
1 vs 3 Ns
2 vs 3 S
1 vs 2 S
1 vs 3 Ns
2 vs 3 S
1 vs 2 S
1 vs 3 Ns
2 vs 3 S
1 vs 2 S
1 vs 3 Ns
2 vs 3 S
1 vs 2 S
1 vs 3 S
2 vs 3 NS
1 vs 2 S
1 vs 3 S
2 vs 3NS
1 vs 2 Ns
1 vs 3 Ns
2 vs 3 Ns
120
100
Figure 2: Showing mean heart rate values at different times
80
60
40
Group DEX
20
Group SNP
Group ESM
The operative field conditions were significantly better in the DEX group than the SNP and ESM group
(though better in ESM group than SNP group) at 15, 30, 45 and 60 min after beginning of the surgery (Fig. 3).
DOI: 10.9790/0853-14107126131
www.iosrjournals.org
129 | Page
Comparison of Dexmedetomidine, Esmolol and Sodium Nitroprusside for Hypotensive Anaesthesia...
4
Figure3: Quality of operative field evaluated using the quality
3.5
3
2.5
Group DEX
Group SNP
1.5
Group ESM
1
0.5
0
5 Min
15 Min 30 Min 45 Min 60 Min 75 Min
End of surgery
The total dose of fentanyl was significantly lower in theDEX group in comparison with the SNP and
ESM groups[2.4 (0.31) vs. 4.4(0.40) vs4.3 (0.37) mg/kg,) respectively, P =0.001] (Table 4).
Time to first rescue analgesia was statistically significant shorter in the SNP and ESM groups than in
the DEX group (P = 0.001) (Table 4).
Table 4:- Total dose of intraoperative fentanyl and postoperativetime of rescue analgesia in each group
Group 1(DEX)
2.3(0.31)
49.50(8.74)
Fentanyl g/kg
Time of first rescue
analgesia (min)
Group 2(SNP)
4.4(0.40)
23.47(9.54)
Group 3(ESM)
4.3(0.37)
25.32(8.76)
P value
0.001
0.001
The mean postoperative sedation scores were significantly lower in SNP and ESM groups than in DEX
group at 15 min and at 30 min. (P<0.01). No significant difference was observed in sedation score at 60 min in
all the groups and in all the groups no patient complained of any sign of awareness.
Table 5:-Recovery characteristics and sedation scores
Emergence time min
Time to modified Aldrete
score 9 min
Sedation score 15 min after
surgery
Sedation score 30 min after
surgery
Sedation score 60 min after
surgery
Group 1(DEX)
7.02.0**
10.01.9**
Group 2(SNP)
4.31.6
8.11.5
Group 3(ESM)
4.62.4
8.21.3
3.90.6**
2.40.5
2.30.6
3.30.3**
2.30.6
2.10.3
2.70.2
2.10.3
2.00.5
** highly significant
IV.
Discussion
Numerous studies have been performed till date to compare the efficacy of hypotensive agents of
different classes in FESS. In our study it was observed that the efficacy of dexmedetomidine as hypotensive
agent was better esmolol and sodium nitroprusside in FESS.
Sodium nitroprusside is a direct acting vasodilator which acts as vascularsmooth muscles.The net
result of vasodilatation and increased cardiac output is increased blood flow through the mucous membrane
capillaries and increased bleeding during surgery on mucous membranes therefore not improving surgical
conditions.
Esmolol is a short acting 1 adrenoceptor antagonist[5]and hypotension caused by it results in
increased sympathetic tone of the mucous membrane arterioles that exert unopposed adrenergic effects on the
mucous membrane vasculature,causing capillary vasoconstriction and reduced bleeding[6].
Dexmedetomidine, an S-enantiomer of medetomidine is an2 adrenergic agonist[7].Ithas got
sedative,analgesic, anxiolytic and sympatholytic effects that blunt many of the responses in perioperative
period.It reduces the requirements for volatile anaesthetics,sedatives and analgesicswithout causing significant
respiratory depression[8].It causes hypotension due toits sympatholytic effect.It decreases heart rate,cardiac
DOI: 10.9790/0853-14107126131
www.iosrjournals.org
130 | Page
Comparison of Dexmedetomidine, Esmolol and Sodium Nitroprusside for Hypotensive Anaesthesia...
output,mean arterial pressure and norepinephrine release.All these parameters together lead to significantly
reduced bleeding and better surgical conditions.
In our study it was observed that bleeding was much less with better hemodynamic in
dexmedetomidine group as compared to esmolol and sodium nitroprusside group.The efficacy of
dexmedetomidine in providing better surgical field and less blood loss in controlled hypotension has been
observed in other studies[9,10].
Richa et al.,[11] reported that extubation time was significantly slower in patients receiving
dexmedetomidine compared with those receiving remifentanyl for controlled hypotension. In the present study
patients of DEX group had significant higher postoperative sedation scores than those in SNP and ESM groups.
Dexmedetomidine has sedative and analgesic sparing effects via central actions in the locus ceruleus and in the
dorsal horn of the spinal cord.[12]
The less intraoperative need for fentanyl in the DEX group than the SNP group is in agreement with
the result of Gurbet et al. [13], who reported that an intraoperative infusion of DEX reduces the perioperative
analgesic requirement. The delayed requirement of postoperative rescue analgesia in the DEX group in
comparison with the SNP group is because of the analgesic effect of DEX, which has been reported in another
study of Dogan et al. [14], who found less postoperative pain in septoplasty performed under local anesthesia
and DEX sedation than general anesthesia.
It was also observed that among sodium nitroprusside and esmolol group, esmolol resulted in lesser
blood loss than sodium nitroprusside.
V.
Conclusion
It can be concluded from our study that dexmedetomidine is an effective hypotensive agent and results
in stable hemodynamics than esmolol and sodium nitroprusside in FESS.Compared with SNP and ESM, it has
the advantage of reduced blood loss and more stable hemodynamics. In addition, it exerts inherent analgesic and
anaesthetic effects. Further studies of the hypotensive effect, intraoperative and postoperative antalgic effects of
DEX during various types of surgery are required.
References
[1].
[2].
[3].
[4].
[5].
[6].
[7].
[8].
[9].
[10].
[11].
[12].
[13].
[14].
[15].
Ankit Patel, MD; Chief Editor: Arlen D Meyers, MD, MBA;Functional endoscopic sinus surgery overview Updated December
14,2014
Andre P.Boezaart,Johan van der Merwe,AndreCoetzee.Comparison of sodium nitroprusside and esmolol-induced controlled
hypotension for functional endoscopic sinus surgery.Canadian journal of anaesthesia 1995/42:5/pp 373-6
ATobias JD. Controlled hypotension in children: A critical review of available agents.PaediatrDrugs.2002;4:439453.
ElGohary MM, Arafa AS. Dexmedetomidine as a hypotensive agent: efficacyand hemodynamic response during spinal surgery for
idiopathic scoliossis inadolescents. Egypt J Anesth 2010; 26:305311.
Blowey DL. Antihypertensive agents: Mechanisms of action, safety profiles, and current uses inchildren. CurrTher Res Clin Exp.
2001;62:298313.
IclalOzdemirKol, MD1; KenanKaygusuz, MD1; AltanYildirim, MD2;
Mansur Dogan, MD2; SinanGursoy, MD1; EvrenYucel, MD1; andCaner Mimaroglu, MD1Controlled Hypotension WithDesflurane
CombinedWith Esmolol or Dexmedetomidine DuringTympanoplasty in Adults: A Double-Blind,Randomized, Controlled
Trial;currentthereupetic researchVolume 70, Number 3, June 2009
Cormack JR, Orme RM, Costello TG (2005). "The role of alpha2-agonists in neurosurgery". Journal of Clinical
Neuroscience 12 (4): 3758. doi:10.1016/j.jocn.2004.06.008. PMID 15925765
Paris A, Tonner PH (2005). "Dexmedetomidine in anaesthesia". Current Opinion in Anaesthesiology 18 (4): 412
8. doi:10.1097/01.aco.0000174958.05383.d5.PMID 16534267.
Durmus M, But AK, Dogan Z, Yucel A, Miman MC, Ersoy MO. Effect ofdexmedetomidine on bleeding during tympanoplasty or
septorhinoplasty. EurJ Anaesthesiol 2007; 24:447453.
Ayoglu H, Yapakci O, Ugur MB, Uzun L, Altunkaya H, Ozer Y, et al. Effectivenessof dexmedetomidine in reducing bleeding
during septoplasty andtympanoplasty operations. J ClinAnesth.
Richa F, Yazigi A, Sleilaty G, Yazbeck P. Comparison between dexmedetomidine and remifentanil for controlled hypotension
during tympanoplasty. Eur J Anaesthesiol. 2008;25:36974. [PubMed]
Guo TZ, Jiang JY, Buttermann AE, Maze M. Dexmedetomidine injection into the locus coeruleus produces antinociception.
Anesthesiology. 1996;84:87381. [PubMed]
Gurbet A, Basagan-Mogol E, Turker G, Ugun F, Kaya FN, Ozcan B. Intraoperative infusion of dexmedetomidine reduces
perioperative analgesic requirements. Can J Anaesth 2006; 53:646652.
Dogan R, Erbek S, Gonencer HH, Erbek HS, Isbilen C, Arslan G. Comparison of local anaesthesia with dexmedetomidine sedation
and general anaesthesia during septoplasty. Eur J Anaesthesiol 2010; 27:960964.
DOI: 10.9790/0853-14107126131
www.iosrjournals.org
131 | Page
Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Attitude and Perceptions of University Students in Zimbabwe Towards HomosexualityDokumen5 halamanAttitude and Perceptions of University Students in Zimbabwe Towards HomosexualityInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- "I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweDokumen5 halaman"I Am Not Gay Says A Gay Christian." A Qualitative Study On Beliefs and Prejudices of Christians Towards Homosexuality in ZimbabweInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Socio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanDokumen7 halamanSocio-Ethical Impact of Turkish Dramas On Educated Females of Gujranwala-PakistanInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Role of Extrovert and Introvert Personality in Second Language AcquisitionDokumen6 halamanThe Role of Extrovert and Introvert Personality in Second Language AcquisitionInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- A Review of Rural Local Government System in Zimbabwe From 1980 To 2014Dokumen15 halamanA Review of Rural Local Government System in Zimbabwe From 1980 To 2014International Organization of Scientific Research (IOSR)Belum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- A Proposed Framework On Working With Parents of Children With Special Needs in SingaporeDokumen7 halamanA Proposed Framework On Working With Parents of Children With Special Needs in SingaporeInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Impact of Technologies On Society: A ReviewDokumen5 halamanThe Impact of Technologies On Society: A ReviewInternational Organization of Scientific Research (IOSR)100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Comparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesDokumen7 halamanComparative Visual Analysis of Symbolic and Illegible Indus Valley Script With Other LanguagesInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Assessment of The Implementation of Federal Character in Nigeria.Dokumen5 halamanAssessment of The Implementation of Federal Character in Nigeria.International Organization of Scientific Research (IOSR)Belum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Investigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehDokumen4 halamanInvestigation of Unbelief and Faith in The Islam According To The Statement, Mr. Ahmed MoftizadehInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- An Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyDokumen14 halamanAn Evaluation of Lowell's Poem "The Quaker Graveyard in Nantucket" As A Pastoral ElegyInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Edward Albee and His Mother Characters: An Analysis of Selected PlaysDokumen5 halamanEdward Albee and His Mother Characters: An Analysis of Selected PlaysInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Relationship Between Social Support and Self-Esteem of Adolescent GirlsDokumen5 halamanRelationship Between Social Support and Self-Esteem of Adolescent GirlsInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Role of Madarsa Education in Empowerment of Muslims in IndiaDokumen6 halamanRole of Madarsa Education in Empowerment of Muslims in IndiaInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- Designing of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesDokumen5 halamanDesigning of Indo-Western Garments Influenced From Different Indian Classical Dance CostumesIOSRjournalBelum ada peringkat
- Importance of Mass Media in Communicating Health Messages: An AnalysisDokumen6 halamanImportance of Mass Media in Communicating Health Messages: An AnalysisInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Topic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshDokumen7 halamanTopic: Using Wiki To Improve Students' Academic Writing in English Collaboratively: A Case Study On Undergraduate Students in BangladeshInternational Organization of Scientific Research (IOSR)Belum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- 3energy Balance Approach - Griffith TheoryDokumen39 halaman3energy Balance Approach - Griffith TheoryMohd_Safuan_Ma_4863Belum ada peringkat
- OFF2328 - Project - Travel ItineraryDokumen3 halamanOFF2328 - Project - Travel Itineraryalisaoud55555Belum ada peringkat
- T&D FinalDokumen69 halamanT&D Finalthella deva prasadBelum ada peringkat
- Ebop Scada ManualDokumen41 halamanEbop Scada ManualDawood TahirBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Prep 2015Dokumen792 halamanPrep 2015Imran A. IsaacBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- WHLP12 Quarter 1Dokumen8 halamanWHLP12 Quarter 1rhaineBelum ada peringkat
- Chapter 2Dokumen63 halamanChapter 2Mohammad ja'farBelum ada peringkat
- 13.8v Power Supply PS HighCurrentDokumen17 halaman13.8v Power Supply PS HighCurrentMadumathi BulumullaBelum ada peringkat
- R 2 KyDokumen3 halamanR 2 KyJorge AzurduyBelum ada peringkat
- Fault Codes VauxhallDokumen7 halamanFault Codes VauxhallMatt DuffillBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Opportunistic Parasitic InfectionsDokumen57 halamanOpportunistic Parasitic Infectionstummalapalli venkateswara raoBelum ada peringkat
- Title 250706Dokumen556 halamanTitle 250706callmeasthaBelum ada peringkat
- Dont Pay With Itunes Gift Cards FinalDokumen1 halamanDont Pay With Itunes Gift Cards FinalJack WilliamsBelum ada peringkat
- Estimating For Heavy Construction and Unit Price BidsDokumen77 halamanEstimating For Heavy Construction and Unit Price BidsYousaf MulattuBelum ada peringkat
- Technical Data: Rotax Kart Type R1, Model 2002Dokumen2 halamanTechnical Data: Rotax Kart Type R1, Model 2002Gallego VilaBelum ada peringkat
- Chapter 5 Emerging Modes - 1.2Dokumen91 halamanChapter 5 Emerging Modes - 1.2TARNISH HAREE NJBelum ada peringkat
- Electric Bike BatteryDokumen3 halamanElectric Bike BatteryOrganic MechanicBelum ada peringkat
- Algebra 2 and Trigonometry: English Bengali Problem SolvingDokumen13 halamanAlgebra 2 and Trigonometry: English Bengali Problem SolvingHasan AsifBelum ada peringkat
- Freckle Juice - Activity PackageDokumen5 halamanFreckle Juice - Activity Packagekristyalb100% (1)
- Chapter 1Dokumen43 halamanChapter 1arun neupaneBelum ada peringkat
- P&H - 320XPCDokumen8 halamanP&H - 320XPCClider Niño100% (2)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Leontief PDFDokumen7 halamanLeontief PDFErvin ArrasyidBelum ada peringkat
- Valeroso vs. CA Case DigestDokumen1 halamanValeroso vs. CA Case DigestMarivic Veneracion100% (2)
- Development of A Belt Conveyor For Small Scale Industry: Journal of Advancement in Engineering and TechnologyDokumen5 halamanDevelopment of A Belt Conveyor For Small Scale Industry: Journal of Advancement in Engineering and TechnologyMuhammad Salman KhanBelum ada peringkat
- Leps202 PDFDokumen20 halamanLeps202 PDFSoma NaikBelum ada peringkat
- Using Transistor As A Switch - ErmicroblogDokumen24 halamanUsing Transistor As A Switch - ErmicroblogRKMBelum ada peringkat
- Alkhairat Company Profile (Final) Kii LamaadDokumen28 halamanAlkhairat Company Profile (Final) Kii LamaadAbdulkadir HusseinBelum ada peringkat
- EPGP-13-Quality Managment - Course Outline - Sec A, B, CDDokumen4 halamanEPGP-13-Quality Managment - Course Outline - Sec A, B, CDreva_radhakrish1834Belum ada peringkat
- Format. Hum - The Right To Privacy Is Protected As An Intrinsic Part of The Right To Life and Personal Liberty Under Article 21 of The Constitution of India An EvaluationDokumen12 halamanFormat. Hum - The Right To Privacy Is Protected As An Intrinsic Part of The Right To Life and Personal Liberty Under Article 21 of The Constitution of India An EvaluationImpact JournalsBelum ada peringkat
- Manual de Operación Terrometro de GanchoDokumen19 halamanManual de Operación Terrometro de GanchoIsrael SanchezBelum ada peringkat
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionDari EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionPenilaian: 4 dari 5 bintang4/5 (404)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedDari EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedPenilaian: 4.5 dari 5 bintang4.5/5 (82)
- The Age of Magical Overthinking: Notes on Modern IrrationalityDari EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityPenilaian: 4 dari 5 bintang4/5 (35)