Anda mungkin juga menyukai
- Critical Soft-Tissue Dimensions With Dental Implantsand Treatment Concepts PDFDokumen13 halamanCritical Soft-Tissue Dimensions With Dental Implantsand Treatment Concepts PDFgirl33Belum ada peringkat
- Sinus Floor Elevation Utilizing The PDFDokumen13 halamanSinus Floor Elevation Utilizing The PDFgirl33Belum ada peringkat
- Zygomatic Implants PDFDokumen18 halamanZygomatic Implants PDFgirl33Belum ada peringkat
- Short Implant in Limited Bone Volume PDFDokumen25 halamanShort Implant in Limited Bone Volume PDFgirl330% (1)
- Neurovascular Disturbances After Implant Surgery PDFDokumen15 halamanNeurovascular Disturbances After Implant Surgery PDFgirl33Belum ada peringkat
- Implant-Assisted Complete Prostheses PDFDokumen13 halamanImplant-Assisted Complete Prostheses PDFgirl33Belum ada peringkat
- Management of Peri-Implant Mucositis and Peri-Implantitis PDFDokumen19 halamanManagement of Peri-Implant Mucositis and Peri-Implantitis PDFgirl33Belum ada peringkat
- Orto Bun 3Dokumen12 halamanOrto Bun 3girl33Belum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Impact of Drug Abuse On Society A Review On Drug Abuse in The Context of SocietyDokumen3 halamanThe Impact of Drug Abuse On Society A Review On Drug Abuse in The Context of SocietyInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Cerebellar StrokeDokumen12 halamanCerebellar StrokewhitecloudsBelum ada peringkat
- Tumors of External EarDokumen10 halamanTumors of External Earsavin1996100% (2)
- ImmunizationDokumen2 halamanImmunizationannamcconkeyBelum ada peringkat
- Chapter 2: Health Promotion in Middle-Aged AdultsDokumen10 halamanChapter 2: Health Promotion in Middle-Aged AdultsTrixie AlvarezBelum ada peringkat
- Temporomandibular Joint Syndrome PDFDokumen4 halamanTemporomandibular Joint Syndrome PDFMaxim BzoviiBelum ada peringkat
- Dialysis in AkiDokumen66 halamanDialysis in Akiwael abodiabBelum ada peringkat
- Beg Talk To Doctor - Unit 1Dokumen66 halamanBeg Talk To Doctor - Unit 1Eliza Cristea OneciBelum ada peringkat
- Adverse Eventsd DefinitionsDokumen30 halamanAdverse Eventsd Definitionsika sartikaBelum ada peringkat
- Turner P. Clinical Guide To Oral Implantology... 3ed 2018Dokumen226 halamanTurner P. Clinical Guide To Oral Implantology... 3ed 2018Daniel EmilevBelum ada peringkat
- 1 - Mattu, Amal ECGsDokumen68 halaman1 - Mattu, Amal ECGsKhan A Reh50% (2)
- Old Age Psychiatry LectureDokumen38 halamanOld Age Psychiatry LectureMo 'Fishpondz' IsmailBelum ada peringkat
- Hsci 360 Long Term Care PPT Revised 9Dokumen23 halamanHsci 360 Long Term Care PPT Revised 9api-249502229Belum ada peringkat
- MK SurgeryDokumen900 halamanMK Surgerybovarep216Belum ada peringkat
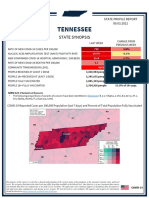
- Tennessee State Profile Report 20210903 PublicDokumen17 halamanTennessee State Profile Report 20210903 PublicAnonymous GF8PPILW5Belum ada peringkat
- Daftar Harga Pengujian Dan Kalibrasi Alat KesehatanDokumen3 halamanDaftar Harga Pengujian Dan Kalibrasi Alat KesehatanVIDYA VIRA PAKSYA PUTRABelum ada peringkat
- About The Dangers of Smoking - 14Dokumen14 halamanAbout The Dangers of Smoking - 14Марта БасішинBelum ada peringkat
- Classification of Acute Pancreatitis-2012 - Revision of The Atlanta Classification and Definitions by International ConsensusDokumen12 halamanClassification of Acute Pancreatitis-2012 - Revision of The Atlanta Classification and Definitions by International ConsensusRichard CuevasBelum ada peringkat
- Serviciile Sociale in Situatii de RiscDokumen15 halamanServiciile Sociale in Situatii de RiscAlina HoaraBelum ada peringkat
- Pediatric Nur Pediatric Nur Pediatric Nur Pediatric Nur Pediatric Nursing Sing Sing Sing SingDokumen10 halamanPediatric Nur Pediatric Nur Pediatric Nur Pediatric Nur Pediatric Nursing Sing Sing Sing Singtheiam772Belum ada peringkat
- All-Cause Mortality and Malaria in African Children: Trends and ControversiesDokumen32 halamanAll-Cause Mortality and Malaria in African Children: Trends and ControversiesBesong MichaelBelum ada peringkat
- Domain 2 Public Health AnnotationsDokumen9 halamanDomain 2 Public Health AnnotationsjkdanielesBelum ada peringkat
- Guidelines Supervised Practice For Limited RegistrationDokumen22 halamanGuidelines Supervised Practice For Limited Registrationمينول بن أحمدBelum ada peringkat
- Reflective Essay Samantha JohnsonDokumen5 halamanReflective Essay Samantha Johnsonapi-329945753Belum ada peringkat
- TheileriaDokumen42 halamanTheileriaMEENU MANOHARBelum ada peringkat
- Management of Facial Fractures1Dokumen279 halamanManagement of Facial Fractures1مهند الوادعيBelum ada peringkat
- Research Paper FinalDokumen7 halamanResearch Paper Finalapi-643588876Belum ada peringkat
- 2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 18-Planning Monitoring and Evaluation of PoliciesDokumen8 halaman2009-SUPPORT Tools For Evidence-Informed Policymaking in Health 18-Planning Monitoring and Evaluation of PoliciesJULIO CESAR MATEUS SOLARTEBelum ada peringkat
- ResumeDokumen5 halamanResumeJuvie Dawn MaquilanBelum ada peringkat
- Name: Prado, Catherine A. Year and Section: BSN III-B Module 4 ReflectionDokumen2 halamanName: Prado, Catherine A. Year and Section: BSN III-B Module 4 ReflectionCatherine PradoBelum ada peringkat