Anda mungkin juga menyukai
- Suarez - Ent EmergenciesDokumen36 halamanSuarez - Ent EmergenciesCarina SuarezBelum ada peringkat
- Principles of Tissue Biopsy in Oral and MaxillofacialDokumen34 halamanPrinciples of Tissue Biopsy in Oral and MaxillofacialEdmond Apriza DrgBelum ada peringkat
- Midface FracturesDokumen31 halamanMidface FracturesJoyabrata SarkarBelum ada peringkat
- Patient Case PresentationDokumen7 halamanPatient Case Presentationapi-616350168Belum ada peringkat
- Uterus Body Pathology: Dr. Mona RashedDokumen29 halamanUterus Body Pathology: Dr. Mona RashedSavin PetersBelum ada peringkat
- The Ultimate BLS CheatsheetDokumen30 halamanThe Ultimate BLS CheatsheetAimee Eichler100% (2)
- 6 Cognitive Behavioral Therapy Techniques For Bipolar DisorderDokumen7 halaman6 Cognitive Behavioral Therapy Techniques For Bipolar Disorderprabha50% (2)
- Acute Cholangitis - AMBOSSDokumen14 halamanAcute Cholangitis - AMBOSSMdacBelum ada peringkat
- Complete Class NotesDokumen83 halamanComplete Class NotesOlivia MaoBelum ada peringkat
- Aneurysmal Bone Cyst of The Zygomatic Arch Causing Limited Mouth OpeningDokumen7 halamanAneurysmal Bone Cyst of The Zygomatic Arch Causing Limited Mouth OpeningAnonymous p28Tktgl5Belum ada peringkat
- Anatomy of The Nose and Sinus Paranasal, Case RhinosinusitisDokumen51 halamanAnatomy of The Nose and Sinus Paranasal, Case RhinosinusitisDera Seta SaputriBelum ada peringkat
- Special Health Reports - Harvard HealthDokumen9 halamanSpecial Health Reports - Harvard HealthBassuBelum ada peringkat
- Vulnerable PopulationsDokumen5 halamanVulnerable Populationsapi-250046004100% (1)
- Related Documents - CREW: Department of State: Regarding International Assistance Offers After Hurricane Katrina: Saudi Arabia AssistanceDokumen81 halamanRelated Documents - CREW: Department of State: Regarding International Assistance Offers After Hurricane Katrina: Saudi Arabia AssistanceCREWBelum ada peringkat
- Esophagus Surgery Lectures: Anatomy, Physiology, Diseases & TreatmentsDokumen22 halamanEsophagus Surgery Lectures: Anatomy, Physiology, Diseases & Treatmentsj,007Belum ada peringkat
- No Aging in India Alzheimer 039 S The Bad Family and Other Modern ThingsDokumen398 halamanNo Aging in India Alzheimer 039 S The Bad Family and Other Modern Thingspria1988Belum ada peringkat
- Grobstein - The Breast Cancer Book - What You Need To Know To Make Informed Decisions (Yale University Press Health & Wellness) - Yale University Press (2005)Dokumen230 halamanGrobstein - The Breast Cancer Book - What You Need To Know To Make Informed Decisions (Yale University Press Health & Wellness) - Yale University Press (2005)Alejandro Vázquez del MercadoBelum ada peringkat
- AAO NHS Ethical Rules For Otolaryngologists 1996Dokumen25 halamanAAO NHS Ethical Rules For Otolaryngologists 1996Mike AdamsBelum ada peringkat
- Geriatric OtolaryngologyDokumen26 halamanGeriatric OtolaryngologySari RakhmawatiBelum ada peringkat
- Determinationof Medicolegalcausation: J. Mark Melhorn,, Marjorie Eskay-AuerbachDokumen11 halamanDeterminationof Medicolegalcausation: J. Mark Melhorn,, Marjorie Eskay-AuerbachSillvia RozzaBelum ada peringkat
- Primary Haemangioma of The Skull: Case ReviewDokumen3 halamanPrimary Haemangioma of The Skull: Case ReviewSoemantri Doank100% (1)
- A History of Pituitary SurgeryDokumen10 halamanA History of Pituitary SurgeryhelbertpalmieroBelum ada peringkat
- Law of Commerce PDFDokumen124 halamanLaw of Commerce PDFSayed Sharif HashimiBelum ada peringkat
- Dental Records by DDUDokumen8 halamanDental Records by DDUpappandairaj100% (1)
- Elements of a Crime ExplainedDokumen12 halamanElements of a Crime ExplainedCP Ispat Unit IIBelum ada peringkat
- Pankaj Das - Aarogyam 1.2 + FBSDokumen10 halamanPankaj Das - Aarogyam 1.2 + FBSplasmadragBelum ada peringkat
- 8 - Member Goodies V 1.2Dokumen1 halaman8 - Member Goodies V 1.2HenoAlambreBelum ada peringkat
- Facial PlasticsDokumen116 halamanFacial Plasticssyed imdadBelum ada peringkat
- Before Smallpox Was Eradicated 0.2Dokumen4 halamanBefore Smallpox Was Eradicated 0.2Kate MartinBelum ada peringkat
- Lip Reconstruction Techniques for Defect RepairDokumen23 halamanLip Reconstruction Techniques for Defect RepairJezreel Ortiz AscenciónBelum ada peringkat
- Macrocytic Anemia - Megaloblastic AnemiaDokumen42 halamanMacrocytic Anemia - Megaloblastic AnemiaDarien LiewBelum ada peringkat
- Plastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic SurgeryDokumen23 halamanPlastic Surgery: Volume 3: Craniofacial, Head and Neck Surgery and Pediatric Plastic SurgeryTugce InceBelum ada peringkat
- Kiminori Sato (Auth.) - Functional Histoanatomy of The Human Larynx-Springer Singapore (2018) PDFDokumen334 halamanKiminori Sato (Auth.) - Functional Histoanatomy of The Human Larynx-Springer Singapore (2018) PDFMdacBelum ada peringkat
- Acute Pyelonephritis in AdultsDokumen12 halamanAcute Pyelonephritis in AdultsviinysantosBelum ada peringkat
- 1986 Book HeadAndNeckManagementOfTheCancDokumen520 halaman1986 Book HeadAndNeckManagementOfTheCancMohamed AlaaBelum ada peringkat
- Ductal Carcinoma in Situ of The BreastDokumen2 halamanDuctal Carcinoma in Situ of The BreastGil LedermanBelum ada peringkat
- Dental Health and Overall Health4Dokumen3 halamanDental Health and Overall Health4Adinda Vashia OktegiandaBelum ada peringkat
- Lecture 1 Historical Aspects of Surgery (Core)Dokumen27 halamanLecture 1 Historical Aspects of Surgery (Core)Charwinth KankaBelum ada peringkat
- Cardiopulmonary AssessmentDokumen22 halamanCardiopulmonary AssessmentMandeep Jangra100% (1)
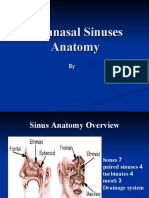
- Paranasal Sinuses AnatomyDokumen55 halamanParanasal Sinuses AnatomyVictor EnachiBelum ada peringkat
- Return To Grand Rounds IndexDokumen14 halamanReturn To Grand Rounds IndexEvyarosna SinagaBelum ada peringkat
- Umbilical Vein CatheterizationDokumen3 halamanUmbilical Vein CatheterizationrohitBelum ada peringkat
- Genetic Crossroads: The Middle East and the Science of Human HeredityDari EverandGenetic Crossroads: The Middle East and the Science of Human HeredityBelum ada peringkat
- Step-By-Step Approach To Endoscopic Cadaveric DissectionDokumen205 halamanStep-By-Step Approach To Endoscopic Cadaveric DissectionJavier Gutiérrez CastilloBelum ada peringkat
- Ethics in DentistryDokumen45 halamanEthics in DentistryMaryam KardoustBelum ada peringkat
- History of SurgeryDokumen35 halamanHistory of SurgeryImolaBakosBelum ada peringkat
- Rise of Modern Surgery OrigiDokumen46 halamanRise of Modern Surgery OrigiPriyanka KaranamBelum ada peringkat
- BarotraumaDokumen15 halamanBarotraumaEfa YusufBelum ada peringkat
- History of RhinoplastyDokumen9 halamanHistory of RhinoplastySyamsul RizalBelum ada peringkat
- Oral MedicineDokumen174 halamanOral Medicineindah100% (1)
- 7th AJCC Staging SCCDokumen9 halaman7th AJCC Staging SCCKambing KatroBelum ada peringkat
- Afd 100617 042Dokumen14 halamanAfd 100617 042Mossad NewsBelum ada peringkat
- 1-History of Surgery in UkraineDokumen16 halaman1-History of Surgery in UkraineErdemBelum ada peringkat
- Renaissance Art in Italy (1400-1600Dokumen13 halamanRenaissance Art in Italy (1400-1600Arvin Jay L JaroBelum ada peringkat
- These Men They Call Knights-1Dokumen22 halamanThese Men They Call Knights-1sar originariusBelum ada peringkat
- Polyp DKKDokumen45 halamanPolyp DKKNadya Beatrix Yohanna NapitupuluBelum ada peringkat
- External Ventricular Drainage PDFDokumen2 halamanExternal Ventricular Drainage PDFBarbara100% (1)
- Dental Hygiene and Periodontal DiseaseDokumen7 halamanDental Hygiene and Periodontal Diseaseapi-536835901Belum ada peringkat
- Consequences: ContentsDokumen201 halamanConsequences: ContentsperzaklieBelum ada peringkat
- Hydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic ShockDokumen10 halamanHydrocortisone, Vitamin C, and Thiamine For The Treatment of Severe Sepsis and Septic Shockmmmaw mmBelum ada peringkat
- Anatomy of Paranasal SinusesDokumen8 halamanAnatomy of Paranasal SinusesPavan TenglikarBelum ada peringkat
- Pulmonary and Critical Care MedicineDokumen48 halamanPulmonary and Critical Care MedicineCarlos HernándezBelum ada peringkat
- The Patient's RightsDokumen5 halamanThe Patient's RightsquesterBelum ada peringkat
- The Best Medicine in The World Is Right in Front of YouDokumen41 halamanThe Best Medicine in The World Is Right in Front of YouDonya MaryaBelum ada peringkat
- Regional AnesthesiaDokumen33 halamanRegional Anesthesiashaq545Belum ada peringkat
- Esophegeal CancerDokumen32 halamanEsophegeal CancerShoaib HashmiBelum ada peringkat
- Read Ver Tips For Drafting An Affidavit: Family Law in BC PDFDokumen7 halamanRead Ver Tips For Drafting An Affidavit: Family Law in BC PDFAvelino Garchitorena Alfelor Jr.Belum ada peringkat
- Convention on International Interests in Mobile Equipment - Cape Town TreatyDari EverandConvention on International Interests in Mobile Equipment - Cape Town TreatyBelum ada peringkat
- Diverticular Disease Symptoms and Treatment AMBOSSDokumen17 halamanDiverticular Disease Symptoms and Treatment AMBOSSMdacBelum ada peringkat
- Chronic Pancreatitis Symptoms, Causes & TreatmentDokumen13 halamanChronic Pancreatitis Symptoms, Causes & TreatmentMdacBelum ada peringkat
- Intestinal Ischemia Guide - Causes, Symptoms & TreatmentDokumen13 halamanIntestinal Ischemia Guide - Causes, Symptoms & TreatmentMdacBelum ada peringkat
- Practiceguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866Dokumen7 halamanPracticeguidelines: Received: 4 May 2017 Accepted: 22 May 2017 DOI: 10.1002/hed.24866MdacBelum ada peringkat
- Gooi 2016Dokumen6 halamanGooi 2016MdacBelum ada peringkat
- Acute Appendicitis - AMBOSSDokumen28 halamanAcute Appendicitis - AMBOSSMdacBelum ada peringkat
- Bray Et al-2018-CA A Cancer Journal For Clinicians PDFDokumen31 halamanBray Et al-2018-CA A Cancer Journal For Clinicians PDFSindhy DewiBelum ada peringkat
- AHNS Series - Do You Know Your Guidelines? Lip CancerDokumen5 halamanAHNS Series - Do You Know Your Guidelines? Lip CancerMdacBelum ada peringkat
- Finding What Works in Health Care Standards For Systematic Reviews IOM 2011 PDFDokumen341 halamanFinding What Works in Health Care Standards For Systematic Reviews IOM 2011 PDFVenance BasilBelum ada peringkat
- ASCO Guidelines Head and NeckDokumen24 halamanASCO Guidelines Head and NeckMdacBelum ada peringkat
- 2012 European Thyroid Association Guidelines For Metastatic Medullary Thyroid CancerDokumen10 halaman2012 European Thyroid Association Guidelines For Metastatic Medullary Thyroid CancerMdacBelum ada peringkat
- Laryngectomee GuideDokumen90 halamanLaryngectomee GuideMdacBelum ada peringkat
- Salvage Laryngectomy Following Organ-Preservation TherapyDokumen8 halamanSalvage Laryngectomy Following Organ-Preservation TherapyMdacBelum ada peringkat
- Brown Et Al-2000-Head & NeckDokumen10 halamanBrown Et Al-2000-Head & NeckMdacBelum ada peringkat
- Masa CervicalDokumen9 halamanMasa CervicalMdacBelum ada peringkat
- Class. of Maxillectomy DefectsDokumen10 halamanClass. of Maxillectomy DefectsJASPREETKAUR0410Belum ada peringkat
- Trauma: HX and PE (Adults) : For The EMS Providers, (Prior To Patient'sDokumen3 halamanTrauma: HX and PE (Adults) : For The EMS Providers, (Prior To Patient'sJustine CastilloBelum ada peringkat
- W2 - Consultation Psychiatry in The Community LectureDokumen32 halamanW2 - Consultation Psychiatry in The Community LectureShailendra Pratap SinghBelum ada peringkat
- A1C-2 Whole Blood enDokumen6 halamanA1C-2 Whole Blood enSyahdie FahledieBelum ada peringkat
- Kumpulan Refarat Co-Ass Radiologi FK UntarDokumen15 halamanKumpulan Refarat Co-Ass Radiologi FK UntarErwin DiprajaBelum ada peringkat
- Rice DiseaseDokumen23 halamanRice DiseaseRayge HarbskyBelum ada peringkat
- Biology of The Alveolar Bone - Orthodontic Tissue Regeneration (OTR) PDFDokumen5 halamanBiology of The Alveolar Bone - Orthodontic Tissue Regeneration (OTR) PDFDonald FlorezBelum ada peringkat
- 2022 SCO OneCare PM Prior Auth Table 3.1.2022-1Dokumen15 halaman2022 SCO OneCare PM Prior Auth Table 3.1.2022-1joshnemoBelum ada peringkat
- A Study To Assess The Effectiveness of Planned Teaching Programme Regarding Stem Cells Among Eligible Couples in Selected Areas of AhmedabadDokumen4 halamanA Study To Assess The Effectiveness of Planned Teaching Programme Regarding Stem Cells Among Eligible Couples in Selected Areas of AhmedabadIJAR JOURNALBelum ada peringkat
- HeartSave AED Brochure - SemiDokumen14 halamanHeartSave AED Brochure - SemiJuan Sebastián Sánchez LópezBelum ada peringkat
- Adult Nursing 2 Teaching PlanDokumen5 halamanAdult Nursing 2 Teaching PlanJerilee SoCute WattsBelum ada peringkat
- AphasiaDokumen8 halamanAphasiaapi-308647214Belum ada peringkat
- BREAST CANCER CLINICAL PHARMACY PRESENTATIONDokumen21 halamanBREAST CANCER CLINICAL PHARMACY PRESENTATIONfrankBelum ada peringkat
- Cancer: Get A Cancer Cover of ' 20 Lakhs at Less Than ' 4 / DayDokumen6 halamanCancer: Get A Cancer Cover of ' 20 Lakhs at Less Than ' 4 / DayUtsav J BhattBelum ada peringkat
- Department of Health - Emerging and Re-Emerging Infectious Disease Program - 2011-10-17Dokumen3 halamanDepartment of Health - Emerging and Re-Emerging Infectious Disease Program - 2011-10-17John Oliver Y. MatuguinaBelum ada peringkat
- Diastema Closure PDFDokumen5 halamanDiastema Closure PDFsimon yonathanBelum ada peringkat
- Global Burden of Cardiovascular Disease: Cardiovascular Diseases in IndiaDokumen17 halamanGlobal Burden of Cardiovascular Disease: Cardiovascular Diseases in IndiaSaurabh BhattacharyaBelum ada peringkat
- Generi Life Physician Statement FormDokumen1 halamanGeneri Life Physician Statement FormVennus RacraquinBelum ada peringkat
- Mens Health Checklist For WebpageDokumen1 halamanMens Health Checklist For WebpageParashuram PatilBelum ada peringkat
- Ersoy-Pruritus 5 D Itch ScaleDokumen7 halamanErsoy-Pruritus 5 D Itch ScaleyosefBelum ada peringkat
- Lec 9 Antihuman Globulin TestingDokumen9 halamanLec 9 Antihuman Globulin TestingMelaine Grace Gemoranion GeopanoBelum ada peringkat
- Pathophysiology: Predisposing Factors: Precipitating FactorsDokumen2 halamanPathophysiology: Predisposing Factors: Precipitating FactorsJemsMei Comparativo MensuradoBelum ada peringkat
- Disease Research PaperDokumen6 halamanDisease Research PaperJose PalaciosBelum ada peringkat
- Hypospadias Pathophysiology and Treatment Principles, Not As Recent As We Think.Dokumen2 halamanHypospadias Pathophysiology and Treatment Principles, Not As Recent As We Think.TI Journals PublishingBelum ada peringkat