Anda mungkin juga menyukai
- Spin Doctoring The ResearchDokumen6 halamanSpin Doctoring The ResearchszopfaszBelum ada peringkat
- Lit Review NealeDokumen9 halamanLit Review Nealeapi-726948535Belum ada peringkat
- 1 s2.0 S0266613816000401 MainDokumen8 halaman1 s2.0 S0266613816000401 MainBeth TorresBelum ada peringkat
- Endometriosis-Associated Infertility: Surgery and IVF, A Comprehensive Therapeutic ApproachDokumen8 halamanEndometriosis-Associated Infertility: Surgery and IVF, A Comprehensive Therapeutic ApproachRangga AdityaBelum ada peringkat
- Pregnancy After Caesarean Section: Fewer or Later?: J.J.H. Eijsink, L. Van Der Leeuw-Harmsen and P.J.Q. Van Der LindenDokumen5 halamanPregnancy After Caesarean Section: Fewer or Later?: J.J.H. Eijsink, L. Van Der Leeuw-Harmsen and P.J.Q. Van Der LindenSamuel Albert Andrian SiagianBelum ada peringkat
- Running Head: HEALTH POLICY PAPER 1Dokumen10 halamanRunning Head: HEALTH POLICY PAPER 1api-283540594Belum ada peringkat
- Pone 0054858 PDFDokumen7 halamanPone 0054858 PDFfiameliaaBelum ada peringkat
- Womens Experiences of Childbirth and PosDokumen7 halamanWomens Experiences of Childbirth and PosMirjana14Belum ada peringkat
- The External Version in Modern Obstetrics: An Alternative to Cesarean DeliveryDokumen21 halamanThe External Version in Modern Obstetrics: An Alternative to Cesarean DeliveryCitrast NursyahidahBelum ada peringkat
- Debate GUIDE PDFDokumen8 halamanDebate GUIDE PDFBlesse PateñoBelum ada peringkat
- Friedman EA (2000) : Labor: Clinical Evaluation and Management, P 23, 2nd Ed. New York, Appleton-Century-CroftsDokumen5 halamanFriedman EA (2000) : Labor: Clinical Evaluation and Management, P 23, 2nd Ed. New York, Appleton-Century-CroftsJuliane ItliongBelum ada peringkat
- StratOG Vaginal BreechDokumen17 halamanStratOG Vaginal BreechNalin AbeysingheBelum ada peringkat
- Fertil Ster IlDokumen6 halamanFertil Ster IlAstrina SupandyBelum ada peringkat
- Ijwh 5 811Dokumen8 halamanIjwh 5 811Anonymous ORleRrBelum ada peringkat
- Ultrasound in Prenatal DiagnosisDokumen11 halamanUltrasound in Prenatal DiagnosisValentina Grajales RestrepoBelum ada peringkat
- Laborinduction: Areviewof Currentmethods: Mildred M. RamirezDokumen11 halamanLaborinduction: Areviewof Currentmethods: Mildred M. RamirezRolando DiazBelum ada peringkat
- Articulo EndometriosisDokumen7 halamanArticulo EndometriosisMaIt VeFloBelum ada peringkat
- Research Summar4Dokumen2 halamanResearch Summar4api-238818738Belum ada peringkat
- Anti-Choice Claims About Abortion and Breast CancerDokumen6 halamanAnti-Choice Claims About Abortion and Breast CancerProgressTXBelum ada peringkat
- DP 203Dokumen63 halamanDP 203charu parasherBelum ada peringkat
- HuffmanShwartzSwanson2015 PDFDokumen9 halamanHuffmanShwartzSwanson2015 PDFIrene De La CruzBelum ada peringkat
- Seijmonsbergenschermers 2013Dokumen9 halamanSeijmonsbergenschermers 2013Febyan AbotBelum ada peringkat
- Pi Is 0002937816462733Dokumen6 halamanPi Is 0002937816462733muhammad maadaBelum ada peringkat
- Research Article: Pregnancy Outcome of Multiparous Women Aged Over 40 YearsDokumen4 halamanResearch Article: Pregnancy Outcome of Multiparous Women Aged Over 40 YearsChristine Laurenza SBelum ada peringkat
- Cesarean Delivery After InductionDokumen5 halamanCesarean Delivery After InductionKIBIR TEMESGENBelum ada peringkat
- Vaginal Misoprostol Prior To Insertion of An Intrauterine Device: An RCTDokumen17 halamanVaginal Misoprostol Prior To Insertion of An Intrauterine Device: An RCTIndra Budi PutraBelum ada peringkat
- Jurnal IDokumen24 halamanJurnal IAgustin LindaBelum ada peringkat
- Vaginal ultrasound reduces IUD expulsion rates less than 40 charactersDokumen3 halamanVaginal ultrasound reduces IUD expulsion rates less than 40 charactersAgustin GonzalezBelum ada peringkat
- Home BirthDokumen33 halamanHome BirthMarlon Royo100% (2)
- Induction of Labor and Risk of Postpartum Hemorrhage in Low Risk ParturientsDokumen8 halamanInduction of Labor and Risk of Postpartum Hemorrhage in Low Risk ParturientsRudolf Fernando WibowoBelum ada peringkat
- Endometriosis EurDokumen5 halamanEndometriosis EurReynaldi AbdullahBelum ada peringkat
- PRINT - Decrease Unintended Pregnancy-PIIS0015028214022092Dokumen7 halamanPRINT - Decrease Unintended Pregnancy-PIIS0015028214022092nurBelum ada peringkat
- Interventions For The Prevention of Pain Associated With The Placement of Intrauterine Contraceptives: An Updated ReviewDokumen14 halamanInterventions For The Prevention of Pain Associated With The Placement of Intrauterine Contraceptives: An Updated ReviewLeonardo Daniel MendesBelum ada peringkat
- Drugs in LabourDokumen9 halamanDrugs in LabourWhira CahbaliBelum ada peringkat
- Jurnal Placenta PreviaDokumen9 halamanJurnal Placenta Previasheva25Belum ada peringkat
- PII002822438690167XDokumen11 halamanPII002822438690167XChristian VieryBelum ada peringkat
- Keberhasilan Post SCDokumen12 halamanKeberhasilan Post SCAprilliaBelum ada peringkat
- Declining FertilityDokumen17 halamanDeclining FertilityNanda PerdanaBelum ada peringkat
- Pneumonia and Pregnancy Outcomes: A Nationwide Population-Based StudyDokumen7 halamanPneumonia and Pregnancy Outcomes: A Nationwide Population-Based StudyAdrin Mahmuddin HarahapBelum ada peringkat
- Is Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyDokumen6 halamanIs Fetal Growth Restriction Associated With A More Severe Maternal Phenotype in The Setting of Early Onset Pre-Eclampsia? A Retrospective StudyYessie ErBelum ada peringkat
- Chouinard2019 PDFDokumen8 halamanChouinard2019 PDFanggunBelum ada peringkat
- Application of Ultrasonography in Female Infertility: A Comprehensive ReviewDokumen11 halamanApplication of Ultrasonography in Female Infertility: A Comprehensive ReviewNur Fitryanti Lubis100% (1)
- Hard Arson 2008Dokumen7 halamanHard Arson 2008elda zulkarnainBelum ada peringkat
- Effects of Labor Support On Mothers, Babies, and Birth OutcomesDokumen10 halamanEffects of Labor Support On Mothers, Babies, and Birth OutcomesLuvi AprilianaBelum ada peringkat
- Hum. Reprod.-2001-Tur-2124-9Dokumen0 halamanHum. Reprod.-2001-Tur-2124-9masdipoBelum ada peringkat
- Impact of A Multiple, IVF Birth On Post-Partum Mental Health: A Composite AnalysisDokumen8 halamanImpact of A Multiple, IVF Birth On Post-Partum Mental Health: A Composite AnalysisMirjana14Belum ada peringkat
- Misoprostol Facilitates IUD Insertion in Nulliparous WomenDokumen8 halamanMisoprostol Facilitates IUD Insertion in Nulliparous WomenPutri Nilam SariBelum ada peringkat
- WatermarkDokumen6 halamanWatermarkAna AdamBelum ada peringkat
- Bangresearch 301 RevisedDokumen4 halamanBangresearch 301 Revisedapi-356371162Belum ada peringkat
- The Natural History of The Normal First Stage Of.6 PDFDokumen6 halamanThe Natural History of The Normal First Stage Of.6 PDFreioctabianoBelum ada peringkat
- Low-Risk Planned Caesarean Versus Planned Vaginal Delivery at Term: Early and Late Infantile OutcomesDokumen11 halamanLow-Risk Planned Caesarean Versus Planned Vaginal Delivery at Term: Early and Late Infantile OutcomesEduarda QuartinBelum ada peringkat
- Family History As A Risk Factor For Pelvic Organ Prolapse: Original ArticleDokumen7 halamanFamily History As A Risk Factor For Pelvic Organ Prolapse: Original ArticlepakemainmainBelum ada peringkat
- Ritgen ManueverDokumen2 halamanRitgen ManueverGustavo Gonzalez CabreraBelum ada peringkat
- ContrafactsheetDokumen3 halamanContrafactsheetCBCP for LifeBelum ada peringkat
- Forveps y VacuumDokumen6 halamanForveps y VacuumSaul Gonzalez HernandezBelum ada peringkat
- Parturition Events and Risk of Urinary Incontinence in Later LifeDokumen16 halamanParturition Events and Risk of Urinary Incontinence in Later LifeMutia LailaniBelum ada peringkat
- English Progress Program: Nama: Nurul Hidayah NIM: 21117091Dokumen12 halamanEnglish Progress Program: Nama: Nurul Hidayah NIM: 21117091nurul4hidayah-99Belum ada peringkat
- Getting Pregnant in the 1980s: New Advances in Infertility Treatment and Sex PreselectionDari EverandGetting Pregnant in the 1980s: New Advances in Infertility Treatment and Sex PreselectionBelum ada peringkat
- On Autumn's Wing, A Story of Birth Trauma, Brain Injury and Miracles.Dari EverandOn Autumn's Wing, A Story of Birth Trauma, Brain Injury and Miracles.Belum ada peringkat
- Contraception for the Medically Challenging PatientDari EverandContraception for the Medically Challenging PatientRebecca H. AllenBelum ada peringkat
- P-Stim™ Auricular Electroacupuncture Stimulation Device For Pain ReliefDokumen10 halamanP-Stim™ Auricular Electroacupuncture Stimulation Device For Pain ReliefoanamemoBelum ada peringkat
- TestDokumen1 halamanTestoanamemoBelum ada peringkat
- Journal of Perinatal EducationDokumen3 halamanJournal of Perinatal EducationoanamemoBelum ada peringkat
- Robin Predare Catre MediciDokumen1 halamanRobin Predare Catre MedicioanamemoBelum ada peringkat
- VBAC or Repeat CDokumen26 halamanVBAC or Repeat CoanamemoBelum ada peringkat
- Bagajul de SpitalDokumen1 halamanBagajul de SpitaloanamemoBelum ada peringkat
- Nursing 212 Final Exam Review - Fall 2017Dokumen12 halamanNursing 212 Final Exam Review - Fall 2017Marc LaBarbera100% (1)
- Final Output - Montuerto, Julius Nixell B.Dokumen3 halamanFinal Output - Montuerto, Julius Nixell B.Jayvee Pellazar BernatBelum ada peringkat
- Community Medicine 2022Dokumen8 halamanCommunity Medicine 2022Ashirwad DadeiaBelum ada peringkat
- Dental Auxiliary: Presented By-Sneha Patil (Final Year BDS Student)Dokumen36 halamanDental Auxiliary: Presented By-Sneha Patil (Final Year BDS Student)Mumin RashidBelum ada peringkat
- Managing Drug SupplyDokumen36 halamanManaging Drug SupplyLisna K. RezkyBelum ada peringkat
- OGDokumen385 halamanOGMin MawBelum ada peringkat
- HIV Lecture Handout 2021Dokumen10 halamanHIV Lecture Handout 2021Jimilyn GallowayBelum ada peringkat
- Nursing Informatics (Terminal Requirement 17)Dokumen1 halamanNursing Informatics (Terminal Requirement 17)Lyza MateoBelum ada peringkat
- Mental health and HIV in IndiaDokumen7 halamanMental health and HIV in IndiaAyu RajikanBelum ada peringkat
- Ethics Gtu 301 Final Exam.14.15 1Dokumen2 halamanEthics Gtu 301 Final Exam.14.15 1JebatAl-KelantaniBelum ada peringkat
- Robsons Ten Group Classification of Cesarean Section at A Tertiary Center in NepalDokumen6 halamanRobsons Ten Group Classification of Cesarean Section at A Tertiary Center in NepalgehanathBelum ada peringkat
- 5.Mr Lode Vedonk - Vietnam Oktober 2023Dokumen11 halaman5.Mr Lode Vedonk - Vietnam Oktober 2023Tran Khanh TrangBelum ada peringkat
- DR Moshiri - Class II Correction by Leveraging Molar Rotation - 2Dokumen4 halamanDR Moshiri - Class II Correction by Leveraging Molar Rotation - 2Enea NastriBelum ada peringkat
- Tieraona Low Dog, MD, With and Marc S. Micozzi, MD, PHD (Auth.) - Women's Health in Complementary and Integrative Medicine. A Clinical Guide (2005)Dokumen353 halamanTieraona Low Dog, MD, With and Marc S. Micozzi, MD, PHD (Auth.) - Women's Health in Complementary and Integrative Medicine. A Clinical Guide (2005)Marfu'ah Mar'ahBelum ada peringkat
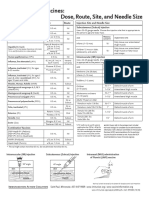
- Injection Site and Needle Size Vaccine Dose RouteDokumen1 halamanInjection Site and Needle Size Vaccine Dose RouteDr Ambana GowdaBelum ada peringkat
- Extension Toxicology Network ExplainedDokumen6 halamanExtension Toxicology Network Explainedjohnrey_lidresBelum ada peringkat
- Overweight 2Dokumen1 halamanOverweight 2Trần NhânBelum ada peringkat
- SLE-CME SlidesDokumen70 halamanSLE-CME Slidesrossi434614Belum ada peringkat
- BJOG - 2023 - Lee - Tranexamic Acid As An Adjunct To Oxytocin Prophylaxis in The Prevention of Postpartum Haemorrhage inDokumen9 halamanBJOG - 2023 - Lee - Tranexamic Acid As An Adjunct To Oxytocin Prophylaxis in The Prevention of Postpartum Haemorrhage inHayfa LayebBelum ada peringkat
- Periodic Health ExamDokumen23 halamanPeriodic Health ExamPernel Jose Alam MicuboBelum ada peringkat
- School Contingency Plan For COVID-19 Pandemic: Department of EducationDokumen14 halamanSchool Contingency Plan For COVID-19 Pandemic: Department of EducationMaria Rose Tariga AquinoBelum ada peringkat
- CV Maggies - HungDokumen4 halamanCV Maggies - HungDoni HardiansyahBelum ada peringkat
- HW 2Dokumen16 halamanHW 2api-371944008Belum ada peringkat
- Torch InfectionsDokumen13 halamanTorch InfectionsOmeBelum ada peringkat
- Ozone Therapy Conference at Bombay Hospital Focuses On Shared ExperiencesDokumen4 halamanOzone Therapy Conference at Bombay Hospital Focuses On Shared ExperiencesDr Saxena Centre for Progressive MedicineBelum ada peringkat
- Medication ReconciliationDokumen9 halamanMedication ReconciliationHoly DishBelum ada peringkat
- CertificateDokumen1 halamanCertificateDrazarBelum ada peringkat
- Clubfoot Deformities ExplainedDokumen3 halamanClubfoot Deformities ExplainedKim GalamgamBelum ada peringkat
- Bayi Baru LahirDokumen43 halamanBayi Baru LahirBRI KUBelum ada peringkat
- NCM 119 Safety Case Study Extended StayDokumen4 halamanNCM 119 Safety Case Study Extended StayMaria Victoria A. PraxidesBelum ada peringkat