Anda mungkin juga menyukai
- Pain Management For Labour and DeliveryDokumen6 halamanPain Management For Labour and DeliveryPujianti LestarinaBelum ada peringkat
- Asam Folat PDFDokumen7 halamanAsam Folat PDFPujianti LestarinaBelum ada peringkat
- Women's Prenatal Concerns Regarding BreastfeedingDokumen6 halamanWomen's Prenatal Concerns Regarding BreastfeedingPujianti LestarinaBelum ada peringkat
- Women's Prenatal Concerns Regarding BreastfeedingDokumen6 halamanWomen's Prenatal Concerns Regarding BreastfeedingPujianti LestarinaBelum ada peringkat
- The Diagnostic Accuracy of External Pelvimetry To Predict Dystocia inDokumen3 halamanThe Diagnostic Accuracy of External Pelvimetry To Predict Dystocia inPujianti LestarinaBelum ada peringkat
- Age-Puberty-Body Dissatisfaction and Physical Activity Decline in Adolescents PDFDokumen45 halamanAge-Puberty-Body Dissatisfaction and Physical Activity Decline in Adolescents PDFPujianti LestarinaBelum ada peringkat
- Hand Hygiene Why How and When BrochureDokumen7 halamanHand Hygiene Why How and When BrochureLeis FatwaBelum ada peringkat
- Assesing The Quality of Last Menstrual Periode DateDokumen12 halamanAssesing The Quality of Last Menstrual Periode DatePujianti LestarinaBelum ada peringkat
- Performance of First Trimester Fetal Ultrasound ScanDokumen12 halamanPerformance of First Trimester Fetal Ultrasound ScanPujianti LestarinaBelum ada peringkat
- Folic Acid Supplementation in Early Second Trimester and The Risk of PreeclampsiaDokumen7 halamanFolic Acid Supplementation in Early Second Trimester and The Risk of PreeclampsiaPujianti LestarinaBelum ada peringkat
- In Utero Physiology Role in Nutrient Delivery and Fetal DevelopmentDokumen4 halamanIn Utero Physiology Role in Nutrient Delivery and Fetal DevelopmentPujianti LestarinaBelum ada peringkat
- Women's Prenatal Concerns Regarding BreastfeedingDokumen6 halamanWomen's Prenatal Concerns Regarding BreastfeedingPujianti LestarinaBelum ada peringkat
- A Comparison of LMP-Based and Ultrasound-Based Estimates of Gestasinal AgeDokumen10 halamanA Comparison of LMP-Based and Ultrasound-Based Estimates of Gestasinal AgePujianti LestarinaBelum ada peringkat
- Comparison of Gestational Age at Birth Based On LMP and USG During 1st TrimesterDokumen10 halamanComparison of Gestational Age at Birth Based On LMP and USG During 1st TrimesterPujianti LestarinaBelum ada peringkat
- KESPRODokumen20 halamanKESPROPryta WidyaningrumBelum ada peringkat
- Labor PositionDokumen71 halamanLabor PositionPujianti LestarinaBelum ada peringkat
- Pujianti Lestarina: PendidikanDokumen4 halamanPujianti Lestarina: PendidikanPujianti LestarinaBelum ada peringkat
- Assessing Progress in LabourDokumen9 halamanAssessing Progress in LabourPujianti LestarinaBelum ada peringkat
- Assessing Progress in LabourDokumen9 halamanAssessing Progress in LabourPujianti LestarinaBelum ada peringkat
- Hands-Knees Labor TrialDokumen10 halamanHands-Knees Labor TrialAnggia PoenyaBelum ada peringkat
- Comfort in Labor Penny SimkinDokumen14 halamanComfort in Labor Penny SimkinPARAMPARUK100% (1)
- A Comparison of LMP-Based and Ultrasound-Based Estimates of Gestasinal AgeDokumen10 halamanA Comparison of LMP-Based and Ultrasound-Based Estimates of Gestasinal AgePujianti LestarinaBelum ada peringkat
- Age Puberty Body Dissatisfaction and Physical Activity Decline in AdolescentsDokumen45 halamanAge Puberty Body Dissatisfaction and Physical Activity Decline in AdolescentsPujianti LestarinaBelum ada peringkat
- Complementary and Alternative Approach For Pain Management in LabourDokumen9 halamanComplementary and Alternative Approach For Pain Management in LabourPujianti LestarinaBelum ada peringkat
- Pain Management During Labour-PharmacologicalDokumen4 halamanPain Management During Labour-PharmacologicalPujianti LestarinaBelum ada peringkat
- Maternal Height and External Pelvimetry To Predict CPDDokumen6 halamanMaternal Height and External Pelvimetry To Predict CPDPujianti LestarinaBelum ada peringkat
- Maternal Positions and Mobility During First Stage Labour - Annemarie Lawrence, Lucy Lewis, G Justus Hofmeyr, Therese Dowswell & Cathy StylesDokumen2 halamanMaternal Positions and Mobility During First Stage Labour - Annemarie Lawrence, Lucy Lewis, G Justus Hofmeyr, Therese Dowswell & Cathy StylesPujianti LestarinaBelum ada peringkat
- Effect of Supplementation During Pregnancy With L-ArginineDokumen8 halamanEffect of Supplementation During Pregnancy With L-ArgininePujianti LestarinaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Leadership Development PlanDokumen5 halamanLeadership Development Planapi-262531856Belum ada peringkat
- Hydralazine For Severe PIHDokumen4 halamanHydralazine For Severe PIHYwagar YwagarBelum ada peringkat
- Vol 19.1 - Sleep Disorders.2013Dokumen252 halamanVol 19.1 - Sleep Disorders.2013Martoiu MariaBelum ada peringkat
- Gardens For Patients With Alzheimer's DiseaseDokumen3 halamanGardens For Patients With Alzheimer's DiseaseKritikou1547Belum ada peringkat
- Spironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabDokumen2 halamanSpironolactone Class Indications: 25MG TAB, 50Mg Tab, 100Mg TabAhmad KusayiriBelum ada peringkat
- Klucel - Varnostni List PDFDokumen4 halamanKlucel - Varnostni List PDFIljuha9Belum ada peringkat
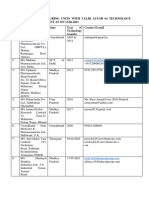
- List of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Dokumen5 halamanList of Manufacturing Units With Valid Ayush 64 Technology Transfer Agreement As On 15.06.2021Sunira EnterprisesBelum ada peringkat
- Minor Surgical Procedures in Maxillofacial SurgeryDokumen65 halamanMinor Surgical Procedures in Maxillofacial SurgerydrzibranBelum ada peringkat
- Dental Anomalies II New PDFDokumen34 halamanDental Anomalies II New PDFFranco Coco SartoriBelum ada peringkat
- Medical DeviceDokumen8 halamanMedical DeviceHarshvardhan ChoudharyBelum ada peringkat
- Archives of Gerontology and GeriatricsDokumen7 halamanArchives of Gerontology and GeriatricsAna ArhipBelum ada peringkat
- Diagnostic Imaging Equipment & Consumables Laser PrintersDokumen5 halamanDiagnostic Imaging Equipment & Consumables Laser Printersnanu_gomezBelum ada peringkat
- Nextier - Pharma 101 - 29-Jun-2016Dokumen28 halamanNextier - Pharma 101 - 29-Jun-2016Ammar ImtiazBelum ada peringkat
- Medical Imaging TechniquesDokumen8 halamanMedical Imaging TechniquesCora DoranBelum ada peringkat
- Iryu.4 Team - Medical.Dragon.E09.720p.Web ENGDokumen45 halamanIryu.4 Team - Medical.Dragon.E09.720p.Web ENGcintoyBelum ada peringkat
- Bioequivalence Comparison Between Two Different Formulations of Alverine AriqDokumen5 halamanBioequivalence Comparison Between Two Different Formulations of Alverine AriqHendri WijayaBelum ada peringkat
- MGR Medical University Medal WinnersDokumen17 halamanMGR Medical University Medal WinnersElavarasanBelum ada peringkat
- Permission To Attend Hockey DayDokumen4 halamanPermission To Attend Hockey Dayapi-244287783Belum ada peringkat
- Oral Hygiene in VentilatorDokumen136 halamanOral Hygiene in VentilatorFelicia Risca RyandiniBelum ada peringkat
- ParoxetineDokumen12 halamanParoxetinemarwa ammarBelum ada peringkat
- Psychological Point of ViewDokumen3 halamanPsychological Point of ViewForam PatelBelum ada peringkat
- Pictorial Review of TI-RADS Scoring System for Thyroid Nodules (38 charactersDokumen1 halamanPictorial Review of TI-RADS Scoring System for Thyroid Nodules (38 charactersmanuel aguilarBelum ada peringkat
- Cardiovascular Physiology Case 9Dokumen50 halamanCardiovascular Physiology Case 9Kim AcostaBelum ada peringkat
- 05thjan Assignment Abroad TimesDokumen8 halaman05thjan Assignment Abroad TimesSameer ShaikBelum ada peringkat
- District Sales Manager in Los Angeles CA Resume Ronald FoxDokumen2 halamanDistrict Sales Manager in Los Angeles CA Resume Ronald FoxRonaldFoxBelum ada peringkat
- Scrotal HerniaDokumen9 halamanScrotal HerniaReymart BolagaoBelum ada peringkat
- Novo NordiskDokumen2 halamanNovo NordiskSpotlightBelum ada peringkat
- Gambaran CT SCAN: (Kasus: Edh, SDH, Ich, Sah, Infark Cerebri, IvhDokumen44 halamanGambaran CT SCAN: (Kasus: Edh, SDH, Ich, Sah, Infark Cerebri, Ivhfahmi rosyadiBelum ada peringkat
- Large Volume Parenterals: Guidelines and Quality Control TestsDokumen36 halamanLarge Volume Parenterals: Guidelines and Quality Control TestsRákêsh MãttàBelum ada peringkat
- Modified Release Dosage FormDokumen24 halamanModified Release Dosage FormSuraj ChoudharyBelum ada peringkat