Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Upramodal Representation of Objects and Actions in The HumanDokumen3 halamanUpramodal Representation of Objects and Actions in The HumanÁngel Carrasco JacomeBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Top-Down Effect of Strategy OnDokumen31 halamanTop-Down Effect of Strategy OnÁngel Carrasco JacomeBelum ada peringkat
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- How to Optimize SEO for Long DocumentsDokumen199 halamanHow to Optimize SEO for Long DocumentsÁngel Carrasco JacomeBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Test Visua de WeschlerDokumen1 halamanTest Visua de WeschlerÁngel Carrasco JacomeBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Visual Perception of Biological Motion and A Model For Its AnalysisDokumen11 halamanVisual Perception of Biological Motion and A Model For Its AnalysisÁngel Carrasco JacomeBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Using Mu Rhythm Desynchronization To Measure Mirror NeuronDokumen10 halamanUsing Mu Rhythm Desynchronization To Measure Mirror NeuronÁngel Carrasco JacomeBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Observed Manipulation of Novel Tools Leads To Mu Rhythm Suppression Over Sensory-Motor CorticesDokumen8 halamanObserved Manipulation of Novel Tools Leads To Mu Rhythm Suppression Over Sensory-Motor CorticesÁngel Carrasco JacomeBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Neural Representation of Observed Actions in The Parietal and Premotor CortexDokumen9 halamanNeural Representation of Observed Actions in The Parietal and Premotor CortexÁngel Carrasco JacomeBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Using Mu Rhythm Desynchronization To Measure Mirror NeuronDokumen10 halamanUsing Mu Rhythm Desynchronization To Measure Mirror NeuronÁngel Carrasco JacomeBelum ada peringkat
- The Effect of Object and Event Orientation On PerceptionDokumen4 halamanThe Effect of Object and Event Orientation On PerceptionÁngel Carrasco JacomeBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Chameleon Effect The Perception-Behavior LinkDokumen18 halamanThe Chameleon Effect The Perception-Behavior LinkÁngel Carrasco JacomeBelum ada peringkat
- Imitation, EmpathyDokumen23 halamanImitation, EmpathyÁngel Carrasco JacomeBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Perception of Motion and QEEG Activity in Human Adults.Dokumen9 halamanPerception of Motion and QEEG Activity in Human Adults.Ángel Carrasco JacomeBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Functional Significance of Mu Rhythms Translating Seeing and Hearing Into DoingDokumen12 halamanThe Functional Significance of Mu Rhythms Translating Seeing and Hearing Into DoingMargarita E. García MoscosoBelum ada peringkat
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Neurophysiology of Human Biological Motion Processing A High-DensityDokumen11 halamanThe Neurophysiology of Human Biological Motion Processing A High-DensityÁngel Carrasco JacomeBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Understanding Action Language Modulates Oscillatory Mu and BetaDokumen7 halamanUnderstanding Action Language Modulates Oscillatory Mu and BetaÁngel Carrasco JacomeBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Cortical Mechanisms of Human ImitationDokumen3 halamanCortical Mechanisms of Human ImitationÁngel Carrasco JacomeBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- Grasping The Intentions of Others With One's Own Mirror Neuron SystemDokumen7 halamanGrasping The Intentions of Others With One's Own Mirror Neuron SystemÁngel Carrasco JacomeBelum ada peringkat
- E. Kohler, C. Keysers, M.A. Umilta, L. Fogassi, V. Gallese, G.Dokumen3 halamanE. Kohler, C. Keysers, M.A. Umilta, L. Fogassi, V. Gallese, G.Ángel Carrasco JacomeBelum ada peringkat
- Journal Pone 0054091Dokumen9 halamanJournal Pone 0054091Anonymous dOg6FYiMJBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Upramodal Representation of Objects and Actions in The HumanDokumen3 halamanUpramodal Representation of Objects and Actions in The HumanÁngel Carrasco JacomeBelum ada peringkat
- EEG Correlates of Action Observation in HumansDokumen8 halamanEEG Correlates of Action Observation in HumansÁngel Carrasco JacomeBelum ada peringkat
- Activation of Human Primary Motor Cortex During ActionDokumen5 halamanActivation of Human Primary Motor Cortex During ActionÁngel Carrasco JacomeBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Action Recogntion in The Premotor CortexDokumen5 halamanAction Recogntion in The Premotor CortexÁngel Carrasco JacomeBelum ada peringkat
- Action RecognitionDokumen19 halamanAction RecognitionÁngel Carrasco JacomeBelum ada peringkat
- Action Observation Activates Premotor and Parietal Areas in A Somatotopic MannerDokumen6 halamanAction Observation Activates Premotor and Parietal Areas in A Somatotopic MannerÁngel Carrasco JacomeBelum ada peringkat
- Casile A, Giese MA. 2006. Non-Visual Motor Learning Influences The Recognition of BiologicalDokumen6 halamanCasile A, Giese MA. 2006. Non-Visual Motor Learning Influences The Recognition of BiologicalÁngel Carrasco JacomeBelum ada peringkat
- Brain Activity During Observation of ActionsDokumen15 halamanBrain Activity During Observation of ActionsÁngel Carrasco JacomeBelum ada peringkat
- Brain Areas Active During VisualDokumen9 halamanBrain Areas Active During VisualÁngel Carrasco JacomeBelum ada peringkat
- Hoffman & Morcom (2018) - Age-Related Changes in The Neural Networks Supporting Semantic Cognition - A Meta-AnalysisDokumen17 halamanHoffman & Morcom (2018) - Age-Related Changes in The Neural Networks Supporting Semantic Cognition - A Meta-Analysisjonas1808Belum ada peringkat
- Spinal AnaesthesiaDokumen4 halamanSpinal Anaesthesiawasis wibowoBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- SELF ASSESSMENT WORKSHEET Class VDokumen5 halamanSELF ASSESSMENT WORKSHEET Class VRashi Ratna BakshBelum ada peringkat
- Bells PalsyDokumen6 halamanBells PalsyElisabeth TikalakaBelum ada peringkat
- NeuropathyDokumen5 halamanNeuropathyAMAN RAJBelum ada peringkat
- Chapter 7 - NERVOUS SYSTEM PDFDokumen58 halamanChapter 7 - NERVOUS SYSTEM PDFMary LimlinganBelum ada peringkat
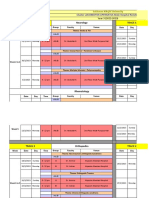
- Sulaiman AlRajhi University Neurology & Orthopedics Hospital Rotation ScheduleDokumen10 halamanSulaiman AlRajhi University Neurology & Orthopedics Hospital Rotation ScheduleAbdullah MelhimBelum ada peringkat
- EEG1Dokumen13 halamanEEG1idno1008Belum ada peringkat
- Early Intervention: Environmental or Experimental Factors The First 5 Years of LifeDokumen55 halamanEarly Intervention: Environmental or Experimental Factors The First 5 Years of Lifeshruti kumar100% (1)
- Topographic Anatomy of Basal NucleiDokumen44 halamanTopographic Anatomy of Basal NucleiRafique AhmedBelum ada peringkat
- Topografska anatomija moždane kore i limbičkih područjaDokumen194 halamanTopografska anatomija moždane kore i limbičkih područjaGoran SimicBelum ada peringkat
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Psychedelic IntegrationDokumen91 halamanPsychedelic IntegrationWhomever me100% (3)
- Neuroplasticity: Presented By: Advincula, Arnina Fortus, Jacyrone Pitpit, MarcusDokumen17 halamanNeuroplasticity: Presented By: Advincula, Arnina Fortus, Jacyrone Pitpit, MarcusCLAIRE DENISSE DEVISBelum ada peringkat
- 21 - Peripheral Nervous SystemDokumen16 halaman21 - Peripheral Nervous Systembhavikrao7605Belum ada peringkat
- Humans use receptors to help them respondDokumen20 halamanHumans use receptors to help them respondshakeel shahulBelum ada peringkat
- Chapt12 LectureDokumen197 halamanChapt12 LecturePye Antwan DelvaBelum ada peringkat
- Hydrocephalus: Mohd Roslee Bin Abd GhaniDokumen44 halamanHydrocephalus: Mohd Roslee Bin Abd GhaniSaha DirllahBelum ada peringkat
- Neurologic NCLEX Practice Test Part 1Dokumen10 halamanNeurologic NCLEX Practice Test Part 1mpasague100% (2)
- Understanding Kundalini Energy and its Role in Spiritual EvolutionDokumen190 halamanUnderstanding Kundalini Energy and its Role in Spiritual Evolutionnityanandroy100% (1)
- Children and Teens With Asperger Syndrome: Instant Help ForDokumen4 halamanChildren and Teens With Asperger Syndrome: Instant Help Foraleksandra_radevicBelum ada peringkat
- Pain Management: Kim L. Paxton MSN, ANP, APRN-BC Bro. Jim O'Brien, OFM, Conv. R.N., M.S.N., O.C.NDokumen69 halamanPain Management: Kim L. Paxton MSN, ANP, APRN-BC Bro. Jim O'Brien, OFM, Conv. R.N., M.S.N., O.C.NsmusquizBelum ada peringkat
- 5 - Friday 800 Am Duhaime Non-Accidental Trauma in Infants and Young ChildrenDokumen6 halaman5 - Friday 800 Am Duhaime Non-Accidental Trauma in Infants and Young ChildrenSantoo VazquezBelum ada peringkat
- Chapter 35: Acute Pain Management: Table 35-1Dokumen32 halamanChapter 35: Acute Pain Management: Table 35-1Tanawat SingboonBelum ada peringkat
- Febrile SeizureDokumen6 halamanFebrile SeizurepipimseptianaBelum ada peringkat
- Neuro Motor Readiness Pl2011Dokumen94 halamanNeuro Motor Readiness Pl2011mohitnet1327100% (3)
- Hering-Breuer ReflexDokumen2 halamanHering-Breuer ReflexNTA UGC-NETBelum ada peringkat
- Physiology of ANS Lecture 1 by Dr. Mudassar Ali RoomiDokumen19 halamanPhysiology of ANS Lecture 1 by Dr. Mudassar Ali RoomiMudassar RoomiBelum ada peringkat
- NIH Public Access: Author ManuscriptDokumen26 halamanNIH Public Access: Author ManuscriptHippokampaBelum ada peringkat
- Anat100 Tutorial 1Dokumen2 halamanAnat100 Tutorial 1Teni LawalBelum ada peringkat
- NURSING CARE PLAN FOR OSTEOARTHRITISDokumen4 halamanNURSING CARE PLAN FOR OSTEOARTHRITISKian HerreraBelum ada peringkat
- Unstoppable You: A Teen Girl's Handbook for Joyful LivingDari EverandUnstoppable You: A Teen Girl's Handbook for Joyful LivingPenilaian: 4.5 dari 5 bintang4.5/5 (21)
- Roxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingDari EverandRoxane Gay & Everand Originals: My Year of Psychedelics: Lessons on Better LivingPenilaian: 5 dari 5 bintang5/5 (4)
- Breaking the Habit of Being YourselfDari EverandBreaking the Habit of Being YourselfPenilaian: 4.5 dari 5 bintang4.5/5 (1454)
- The Guilty Wife: A gripping addictive psychological suspense thriller with a twist you won’t see comingDari EverandThe Guilty Wife: A gripping addictive psychological suspense thriller with a twist you won’t see comingPenilaian: 4 dari 5 bintang4/5 (71)
- Natural Memory Improvement TechniquesDari EverandNatural Memory Improvement TechniquesPenilaian: 4.5 dari 5 bintang4.5/5 (54)
- Tech Detox for Teens: Finding Balance in a Digital WorldDari EverandTech Detox for Teens: Finding Balance in a Digital WorldPenilaian: 4.5 dari 5 bintang4.5/5 (26)
- How to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipDari EverandHow to Talk to Anyone: Learn the Secrets of Good Communication and the Little Tricks for Big Success in RelationshipPenilaian: 4.5 dari 5 bintang4.5/5 (1135)
- Techniques Exercises And Tricks For Memory ImprovementDari EverandTechniques Exercises And Tricks For Memory ImprovementPenilaian: 4.5 dari 5 bintang4.5/5 (40)