Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Approaching Checklist Final PDFDokumen15 halamanApproaching Checklist Final PDFCohort Partnerships100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Architectural Design I: SyllabusDokumen3 halamanArchitectural Design I: SyllabusSrilakshmi PriyaBelum ada peringkat
- Group 4 CariCRIS Case SubmissionDokumen6 halamanGroup 4 CariCRIS Case SubmissionKingsuk MaityBelum ada peringkat
- Creativity and AestheticDokumen17 halamanCreativity and AestheticSyahirah Erahzs100% (1)
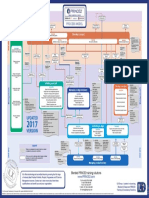
- p2 Process Model 2017Dokumen1 halamanp2 Process Model 2017Miguel Fernandes0% (1)
- The Prodigious MuseDokumen466 halamanThe Prodigious Musesleepyninjitsu100% (1)
- SSPC - Guia 12Dokumen6 halamanSSPC - Guia 12José Alvaro Herrera Ramos50% (2)
- Heirs of Candelaria V RomeroDokumen2 halamanHeirs of Candelaria V Romeromoniquehadjirul100% (1)
- Spanish Web PDFDokumen36 halamanSpanish Web PDFSergio SayagoBelum ada peringkat
- Gender Stereotypes and Performativity Analysis in Norwegian Wood Novel by Haruki Murakami Devani Adinda Putri Reg No: 2012060541Dokumen35 halamanGender Stereotypes and Performativity Analysis in Norwegian Wood Novel by Haruki Murakami Devani Adinda Putri Reg No: 2012060541Jornel JevanskiBelum ada peringkat
- High-Frequency Injection-Based SensorlessDokumen12 halamanHigh-Frequency Injection-Based SensorlessRiad BOUZIDIBelum ada peringkat
- 10 1108 - JKM 01 2020 0064Dokumen23 halaman10 1108 - JKM 01 2020 0064BBA THESISBelum ada peringkat
- Mécanisme de La Physionomie HumaineDokumen2 halamanMécanisme de La Physionomie HumainebopufouriaBelum ada peringkat
- Att.3 Training Evaluation For Course Trainer & FacilitiesDokumen2 halamanAtt.3 Training Evaluation For Course Trainer & FacilitiesYusufBelum ada peringkat
- A Phonological Reconstruction of Proto-ChinDokumen191 halamanA Phonological Reconstruction of Proto-ChinHming Lem100% (1)
- HRM848 Training Techniques and Practices Summer 2021Dokumen39 halamanHRM848 Training Techniques and Practices Summer 2021Dhruvi RajBelum ada peringkat
- Sedition ActDokumen11 halamanSedition ActYei TengBelum ada peringkat
- DSP Setting Fundamentals PDFDokumen14 halamanDSP Setting Fundamentals PDFsamuel mezaBelum ada peringkat
- 3 Murex HIV Ag Ab CombinationDokumen7 halaman3 Murex HIV Ag Ab CombinationElias Dii Rivas GarvanBelum ada peringkat
- CarozziDokumen20 halamanCarozziNicholas Matthew WelshBelum ada peringkat
- Metric Schnorr Lock Washer SpecDokumen3 halamanMetric Schnorr Lock Washer SpecGatito FelinoBelum ada peringkat
- NIA Foundation PLI Proposal Template (Repaired)Dokumen23 halamanNIA Foundation PLI Proposal Template (Repaired)lama dasuBelum ada peringkat
- SDS SheetDokumen8 halamanSDS SheetΠΑΝΑΓΙΩΤΗΣΠΑΝΑΓΟΣBelum ada peringkat
- Pdf-To-Word EditedDokumen48 halamanPdf-To-Word EditedJames Genesis Ignacio LolaBelum ada peringkat
- Reported Speech Rd1Dokumen3 halamanReported Speech Rd1Jose ChavezBelum ada peringkat
- الاستراتيجية الامنية الأمريكيةDokumen141 halamanالاستراتيجية الامنية الأمريكيةAhmedZEMMITBelum ada peringkat
- I. Revised Penal Code (RPC) and Related Special Laws: Riminal AWDokumen11 halamanI. Revised Penal Code (RPC) and Related Special Laws: Riminal AWMc Vharn CatreBelum ada peringkat
- AVERY, Adoratio PurpuraeDokumen16 halamanAVERY, Adoratio PurpuraeDejan MitreaBelum ada peringkat
- Prof Chase B. Wrenn - The True and The Good - A Strong Virtue Theory of The Value of Truth-Oxford University Press (2024)Dokumen196 halamanProf Chase B. Wrenn - The True and The Good - A Strong Virtue Theory of The Value of Truth-Oxford University Press (2024)Mihaela DodiBelum ada peringkat
- Bhagavad Gita Ch.1 Shlok 4++Dokumen1 halamanBhagavad Gita Ch.1 Shlok 4++goldenlion1Belum ada peringkat