Anda mungkin juga menyukai
- Articulo Executive Function & School SuccessDokumen4 halamanArticulo Executive Function & School SuccessadelitaperezBelum ada peringkat
- Aamd Classification 1973Dokumen240 halamanAamd Classification 1973Lusi Anindia RahmawatiBelum ada peringkat
- Occupational Therapy Goals and Obj BankDokumen16 halamanOccupational Therapy Goals and Obj Bankadelitaperez94% (18)
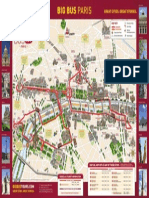
- Big Bus Paris MapsDokumen1 halamanBig Bus Paris MapsadelitaperezBelum ada peringkat
- Category Ot Goals.Dokumen11 halamanCategory Ot Goals.adelitaperez100% (3)
- AOTA Adaptation To Macular Escotomas in Persons With Low VisionDokumen7 halamanAOTA Adaptation To Macular Escotomas in Persons With Low VisionadelitaperezBelum ada peringkat
- Pract I Ce Maki NG Ci RCL Es: Therapyfunzone. ComDokumen1 halamanPract I Ce Maki NG Ci RCL Es: Therapyfunzone. ComadelitaperezBelum ada peringkat
- Hitos Del Desarrollo InglesDokumen6 halamanHitos Del Desarrollo InglesadelitaperezBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Sheath Guidewire Dan CathetersDokumen44 halamanSheath Guidewire Dan CathetersAnip Wungkul100% (1)
- Perdarahan Intra Dan Extra AxialDokumen19 halamanPerdarahan Intra Dan Extra AxialFarmasi FKUNSBelum ada peringkat
- Neuropediatric ExaminationDokumen43 halamanNeuropediatric ExaminationShaniaBelum ada peringkat
- Abstracts and Proceedings WDSC 2009Dokumen110 halamanAbstracts and Proceedings WDSC 2009Rajasree KarunamoorthyBelum ada peringkat
- Buffer Systems in The Body: Protein Buffers in Blood Plasma and CellsDokumen11 halamanBuffer Systems in The Body: Protein Buffers in Blood Plasma and CellsK Jayakumar KandasamyBelum ada peringkat
- The Enigma of Facial Beauty: Esthetics, Proportions, Deformity, and ControversyDokumen6 halamanThe Enigma of Facial Beauty: Esthetics, Proportions, Deformity, and ControversyIsmaelLouGomezBelum ada peringkat
- Dilip K. Ghosh, R. B. Smarta-Pharmaceuticals To Nutraceuticals - A Shift in Disease Prevention-Taylor & Francis - CRC Press (2017)Dokumen274 halamanDilip K. Ghosh, R. B. Smarta-Pharmaceuticals To Nutraceuticals - A Shift in Disease Prevention-Taylor & Francis - CRC Press (2017)davidBelum ada peringkat
- Borax PDFDokumen4 halamanBorax PDFZi LaBelum ada peringkat
- Uv DoseDokumen6 halamanUv DoseRajesh DeshmukhBelum ada peringkat
- Tryptophan Supplement For SleepDokumen35 halamanTryptophan Supplement For SleepZie Dak BlurBelum ada peringkat
- Arthritis Protocol 1Dokumen11 halamanArthritis Protocol 1Co Bay-AgiBelum ada peringkat
- You Will (Probably) Survive Chapter SamplerDokumen28 halamanYou Will (Probably) Survive Chapter SamplerAllen & Unwin100% (1)
- AKUH Kampala Hospital-Press Release - Final - 17 December 2015Dokumen3 halamanAKUH Kampala Hospital-Press Release - Final - 17 December 2015Robert OkandaBelum ada peringkat
- Introductory Lecture Series: The Anesthesia MachineDokumen37 halamanIntroductory Lecture Series: The Anesthesia MachineDenny RamdhanBelum ada peringkat
- 2016 - Lancet StrokeDokumen14 halaman2016 - Lancet StrokeWikler Bernal TorresBelum ada peringkat
- K00.0 K05.0 K00.1 K05.1 K05.2 K01.0 K05.3 K01.1 K05.6 K02.0 K06.0 K02.1 K06.1 K02.2 K06.2 K02.9 K06.9Dokumen1 halamanK00.0 K05.0 K00.1 K05.1 K05.2 K01.0 K05.3 K01.1 K05.6 K02.0 K06.0 K02.1 K06.1 K02.2 K06.2 K02.9 K06.9fitriwijayaBelum ada peringkat
- Read and Choose The Correct Answer From The Box Below.: Boys GirlsDokumen1 halamanRead and Choose The Correct Answer From The Box Below.: Boys GirlsjekjekBelum ada peringkat
- Infertility HysterosDokumen47 halamanInfertility HysterosDenisBelum ada peringkat
- Social Sciences and Applied Social Sciences: Presented By: MS. RICA B. OLIVARDokumen57 halamanSocial Sciences and Applied Social Sciences: Presented By: MS. RICA B. OLIVARJerry De Leon Lpt100% (1)
- The Effects of Skin Bleach in SocietyDokumen8 halamanThe Effects of Skin Bleach in SocietySalma BahBelum ada peringkat
- A Systematic Review of Trunk Restraint TrainingDokumen1 halamanA Systematic Review of Trunk Restraint Traininggans_therapist3321Belum ada peringkat
- Fact Sheet: StutteringDokumen2 halamanFact Sheet: StutteringHaley TutwilerBelum ada peringkat
- Wmh-Cidi Papi Interview: Screening Section (SC)Dokumen9 halamanWmh-Cidi Papi Interview: Screening Section (SC)Monia AzevedoBelum ada peringkat
- Sound TherapyDokumen1 halamanSound TherapyibedaflyBelum ada peringkat
- 2 Articles From Oui Magazine (Feat. Robert Anton Wilson)Dokumen16 halaman2 Articles From Oui Magazine (Feat. Robert Anton Wilson)Jakob AndradeBelum ada peringkat
- Neuroscience: Science of The Brain in PolishDokumen72 halamanNeuroscience: Science of The Brain in PolishInternational Brain Research Organization100% (1)
- Training Table To The Battlefield: Protein Recommendations For WarfightersDokumen4 halamanTraining Table To The Battlefield: Protein Recommendations For WarfightersLalu Reza AldiraBelum ada peringkat
- Association Between Subjective Sleep Quality, Hypertension, Depression and Body Mass Index in A Nigerian Family Practice SettingDokumen7 halamanAssociation Between Subjective Sleep Quality, Hypertension, Depression and Body Mass Index in A Nigerian Family Practice SettingFerdy LainsamputtyBelum ada peringkat
- OmeprazoleDokumen2 halamanOmeprazolephawphawphawBelum ada peringkat
- BC CancerDokumen42 halamanBC CancerIsal SparrowBelum ada peringkat