Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1091)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Periodontology Question BankDokumen44 halamanPeriodontology Question BankVanshika Jain100% (6)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Drake Family - Work SampleDokumen1 halamanDrake Family - Work Sampleapi-248366250Belum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- CHAPTER 8 f4 KSSMDokumen19 halamanCHAPTER 8 f4 KSSMEtty Saad0% (1)
- Recommended Practice For Corrosion Management of Pipelines in Oil & Gas Production and TransportationDokumen123 halamanRecommended Practice For Corrosion Management of Pipelines in Oil & Gas Production and Transportationsaifoa100% (2)
- Rico Short CBCTDokumen14 halamanRico Short CBCTlupusebastianBelum ada peringkat
- EBOOK Rotativ VS Reciproc PDFDokumen10 halamanEBOOK Rotativ VS Reciproc PDFlupusebastianBelum ada peringkat
- Restautation of The Endodontically Treated TeethDokumen109 halamanRestautation of The Endodontically Treated TeethlupusebastianBelum ada peringkat
- Taking Control of Your Practice PhonesDokumen22 halamanTaking Control of Your Practice PhoneslupusebastianBelum ada peringkat
- IRIGANTI The Effects of Temperature On Sodium HypochloriteDokumen4 halamanIRIGANTI The Effects of Temperature On Sodium HypochloritelupusebastianBelum ada peringkat
- Dental Microscope For General DentistryDokumen3 halamanDental Microscope For General DentistrylupusebastianBelum ada peringkat
- Rubber Dam: Presented By: Cheng Yung Yew P11132Dokumen38 halamanRubber Dam: Presented By: Cheng Yung Yew P11132lupusebastianBelum ada peringkat
- Scleroderma PDFDokumen2 halamanScleroderma PDFlupusebastianBelum ada peringkat
- BDJ 2008 152 PDFDokumen5 halamanBDJ 2008 152 PDFlupusebastianBelum ada peringkat
- Surgical Operating Microscopes in Endodontics: Enlarged Vision and PossibilityDokumen5 halamanSurgical Operating Microscopes in Endodontics: Enlarged Vision and PossibilitylupusebastianBelum ada peringkat
- File Application GuideDokumen2 halamanFile Application GuidelupusebastianBelum ada peringkat
- Zeiss ScoDokumen32 halamanZeiss ScolupusebastianBelum ada peringkat
- The Application of Microscopic Surgery in DentistryDokumen6 halamanThe Application of Microscopic Surgery in DentistrylupusebastianBelum ada peringkat
- Ebooks 10 Tips ImplantologyDokumen16 halamanEbooks 10 Tips ImplantologylupusebastianBelum ada peringkat
- Learning Activity Sheet MAPEH 10 (P.E.) : First Quarter/Week 1Dokumen4 halamanLearning Activity Sheet MAPEH 10 (P.E.) : First Quarter/Week 1Catherine DubalBelum ada peringkat
- Main CatalogueDokumen12 halamanMain Catalogueferpa_ferBelum ada peringkat
- PMA 2015 2016 Issue 3 PDFDokumen36 halamanPMA 2015 2016 Issue 3 PDFLyndon Mercado TolentinoBelum ada peringkat
- Occlusal Appliance TherapyDokumen14 halamanOcclusal Appliance TherapyNam BuiBelum ada peringkat
- Intimacy and Healthy Affective Maturaity - Fa-Winter09bDokumen9 halamanIntimacy and Healthy Affective Maturaity - Fa-Winter09bCarlos GiraldoBelum ada peringkat
- Nature and Nurture - How They Play A Role in Serial Killers and THDokumen40 halamanNature and Nurture - How They Play A Role in Serial Killers and THJ.A.B.ABelum ada peringkat
- An Assignment On "Mycology Laboratory Technique"Dokumen1 halamanAn Assignment On "Mycology Laboratory Technique"BsksvdndkskBelum ada peringkat
- City of Atlanta - Structural Checklist: All Items Listed Herein Shall Be Complied With If Applicable To The ProjectDokumen16 halamanCity of Atlanta - Structural Checklist: All Items Listed Herein Shall Be Complied With If Applicable To The ProjectSandip SurBelum ada peringkat
- 1 SMDokumen10 halaman1 SMAnindita GaluhBelum ada peringkat
- FiltrationDokumen22 halamanFiltrationYeabsira WorkagegnehuBelum ada peringkat
- Allison Weech Final ResumeDokumen1 halamanAllison Weech Final Resumeapi-506177291Belum ada peringkat
- Aquamine 50.01Dokumen17 halamanAquamine 50.01Armando RelajoBelum ada peringkat
- IWCF Comb. Supv Equip. 01Dokumen25 halamanIWCF Comb. Supv Equip. 01andrzema100% (3)
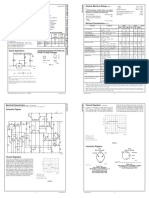
- LM 337Dokumen4 halamanLM 337matias robertBelum ada peringkat
- Toxic RelationshipDokumen1 halamanToxic RelationshipwidyasBelum ada peringkat
- Demolition/Removal Permit Application Form: Planning, Property and Development DepartmentDokumen3 halamanDemolition/Removal Permit Application Form: Planning, Property and Development DepartmentAl7amdlellahBelum ada peringkat
- Celltac MEK 6500Dokumen3 halamanCelltac MEK 6500RiduanBelum ada peringkat
- Krispy Kreme Doughnut Recipe - Immaculate BitesDokumen2 halamanKrispy Kreme Doughnut Recipe - Immaculate Bitesdaisydrops6Belum ada peringkat
- Cataloge ICARDokumen66 halamanCataloge ICARAgoess Oetomo100% (1)
- Nursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDokumen11 halamanNursing Care Plan: Assessment Diagnosis Planning Interventions Rationale EvaluationDa NicaBelum ada peringkat
- Company Catalogue 1214332018Dokumen40 halamanCompany Catalogue 1214332018Carlos FrancoBelum ada peringkat
- Containers HandbookDokumen26 halamanContainers Handbookrishi vohraBelum ada peringkat
- Prepper MealsDokumen22 halamanPrepper MealsmeineanmeldungenBelum ada peringkat
- Alternative ObligationsDokumen42 halamanAlternative ObligationsJanella Gail FerrerBelum ada peringkat
- EE2401 Power System Operation and ControlDokumen93 halamanEE2401 Power System Operation and ControlPrasanth GovindarajBelum ada peringkat