Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- SJCTs Pilot Examination Information & InstructionsDokumen6 halamanSJCTs Pilot Examination Information & InstructionsSkep100% (1)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Vanessa Tarot BookletDokumen36 halamanVanessa Tarot BookletClassic Bobby100% (2)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Russian and US Mind Control Technology Psychotronic WarDokumen123 halamanRussian and US Mind Control Technology Psychotronic WardropsyBelum ada peringkat
- Periodontics PDFDokumen195 halamanPeriodontics PDFدينا حسن نعمة100% (1)
- KLYuChI 2 Kurs-Arakin PDFDokumen159 halamanKLYuChI 2 Kurs-Arakin PDFSayfaBelum ada peringkat
- SASO 1431 (GS 1355) SorbitolDokumen5 halamanSASO 1431 (GS 1355) SorbitolakBelum ada peringkat
- Snodgrass (1980) A Standardized Set of 260 Pictures. Norms For Name Agreement, Image Agreement, Familiarity, and Visual ComplexityDokumen42 halamanSnodgrass (1980) A Standardized Set of 260 Pictures. Norms For Name Agreement, Image Agreement, Familiarity, and Visual ComplexityΜακίν Ξηροί ΚαρποίBelum ada peringkat
- Cardiac MarkersDokumen23 halamanCardiac MarkersAsmaaYLBelum ada peringkat
- The Star News November 20, 2014Dokumen37 halamanThe Star News November 20, 2014The Star NewsBelum ada peringkat
- Daftar PustakaDokumen3 halamanDaftar PustakaErliTa TyarLieBelum ada peringkat
- HO#1.1 Caring For The BodyDokumen7 halamanHO#1.1 Caring For The BodyGemma CanlapanBelum ada peringkat
- Invega Sustenna PIDokumen13 halamanInvega Sustenna PIAisha SyedBelum ada peringkat
- International Congress 1263Dokumen12 halamanInternational Congress 1263AksMastBelum ada peringkat
- Slide PPT PrismaDokumen31 halamanSlide PPT PrismaUlul Azmi AdnanBelum ada peringkat
- Idnt Na MatrixDokumen20 halamanIdnt Na MatrixicalBelum ada peringkat
- LeaP PE G6 Week 1 Q3Dokumen6 halamanLeaP PE G6 Week 1 Q3Rosemarie Mañabo RamirezBelum ada peringkat
- Tugas Jurnal TeksolDokumen6 halamanTugas Jurnal TeksolNovita IndahBelum ada peringkat
- Hyatt Amritsar showcases Chinese and Thai cuisineDokumen1 halamanHyatt Amritsar showcases Chinese and Thai cuisineAnmol MehanBelum ada peringkat
- Bacteriological Water Analysis of Hostel's WaterDokumen12 halamanBacteriological Water Analysis of Hostel's Waterapi-3705267Belum ada peringkat
- PamphletDokumen1 halamanPamphletAldenn MinotaurBelum ada peringkat
- ASCGULF Company: Mohammad Gousu Basha ShaikDokumen3 halamanASCGULF Company: Mohammad Gousu Basha ShaikmohammadgouseBelum ada peringkat
- SolidtumorsinchildrenDokumen24 halamanSolidtumorsinchildrenPriyaBelum ada peringkat
- Exercise Chart: Warm UpDokumen1 halamanExercise Chart: Warm UpJeremy van der MerweBelum ada peringkat
- Burns Guide: Causes, Types, TreatmentDokumen4 halamanBurns Guide: Causes, Types, TreatmentMartin KoaBelum ada peringkat
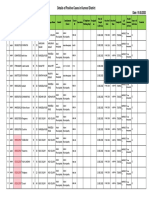
- Details of Positive Cases in Kurnool DistrictDokumen60 halamanDetails of Positive Cases in Kurnool DistrictSohail MullaBelum ada peringkat
- Annex 6: Guidance On Good Manufacturing Practices (GMP) : Inspection ReportDokumen5 halamanAnnex 6: Guidance On Good Manufacturing Practices (GMP) : Inspection Reportumarn1582Belum ada peringkat
- TB Teaching PlanDokumen5 halamanTB Teaching PlanTrisha Fae Loyola Balagot100% (1)
- Hematology Lecture - AnemiaDokumen10 halamanHematology Lecture - AnemiaKimberly EspaldonBelum ada peringkat
- Lection 8 SyphilisDokumen39 halamanLection 8 SyphilisAtawna AtefBelum ada peringkat
- Acd Iam 05 ImatDokumen2 halamanAcd Iam 05 Imatnjk realty100% (1)