Anda mungkin juga menyukai
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (73)
- Flare Finance Ecosystem MapDokumen1 halamanFlare Finance Ecosystem MapEssence of ChaBelum ada peringkat
- NLRB V StarbucksDokumen88 halamanNLRB V StarbucksrkarlinBelum ada peringkat
- NLRB V StarbucksDokumen88 halamanNLRB V StarbucksrkarlinBelum ada peringkat
- 7458-PM Putting The Pieces TogetherDokumen11 halaman7458-PM Putting The Pieces Togethermello06Belum ada peringkat
- ForfeitureDokumen34 halamanForfeiturerkarlinBelum ada peringkat
- Sheperd's Run Draft Ores PermitDokumen92 halamanSheperd's Run Draft Ores PermitrkarlinBelum ada peringkat
- 04 Dasmarinas Vs Reyes GR No 108229Dokumen2 halaman04 Dasmarinas Vs Reyes GR No 108229Victoria Melissa Cortejos PulidoBelum ada peringkat
- Taxation of interest income paid to foreign corporationsDokumen1 halamanTaxation of interest income paid to foreign corporationsCass CataloBelum ada peringkat
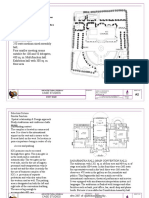
- International Convention Center, BanesworDokumen18 halamanInternational Convention Center, BanesworSreeniketh ChikuBelum ada peringkat
- Alfa Laval Complete Fittings CatalogDokumen224 halamanAlfa Laval Complete Fittings CatalogGraciele SoaresBelum ada peringkat
- Entrepreneurship WholeDokumen20 halamanEntrepreneurship WholeKrizztian SiuaganBelum ada peringkat
- Fra Federal Register RequestDokumen3 halamanFra Federal Register RequestrkarlinBelum ada peringkat
- PSC Order On Inflation AdjustmentDokumen93 halamanPSC Order On Inflation Adjustmentrkarlin100% (1)
- Hunter Tubing LawsuitDokumen5 halamanHunter Tubing LawsuitrkarlinBelum ada peringkat
- Congestion Management Process Report Public ReviewDokumen104 halamanCongestion Management Process Report Public ReviewrkarlinBelum ada peringkat
- Warn Dol ReportDokumen22 halamanWarn Dol ReportrkarlinBelum ada peringkat
- Central Hudson PulpDokumen33 halamanCentral Hudson PulprkarlinBelum ada peringkat
- Norlite V DEC 911182 23 Norlite LLC V Norlite LLC PETITION 1Dokumen9 halamanNorlite V DEC 911182 23 Norlite LLC V Norlite LLC PETITION 1rkarlinBelum ada peringkat
- MWBE FY2223 - DMWBDAnnualReportDokumen20 halamanMWBE FY2223 - DMWBDAnnualReportrkarlinBelum ada peringkat
- Oorah Gun CaseDokumen27 halamanOorah Gun CaserkarlinBelum ada peringkat
- Norlite Health Outcomes Report 09-06-23 3 As PDF 1Dokumen14 halamanNorlite Health Outcomes Report 09-06-23 3 As PDF 1rkarlinBelum ada peringkat
- NYISO 2023 Power TrendsDokumen46 halamanNYISO 2023 Power TrendsrkarlinBelum ada peringkat
- Norlite Decision On Motion To InterveneDokumen10 halamanNorlite Decision On Motion To IntervenerkarlinBelum ada peringkat
- City of Seattle Complaint 012423 FiledDokumen34 halamanCity of Seattle Complaint 012423 FiledrkarlinBelum ada peringkat
- Warn Mid State Raceway Mohawk Valley 2022 0171 5-11-2023Dokumen1 halamanWarn Mid State Raceway Mohawk Valley 2022 0171 5-11-2023rkarlinBelum ada peringkat
- Norlite Dust PlanDokumen182 halamanNorlite Dust PlanrkarlinBelum ada peringkat
- Copake V Ores Appellate DecisionDokumen13 halamanCopake V Ores Appellate DecisionrkarlinBelum ada peringkat
- Advancing NY Clean Energy Seven PrincipalsDokumen8 halamanAdvancing NY Clean Energy Seven PrincipalsrkarlinBelum ada peringkat
- New York Supreme Court: Appellate Division-Third DepartmentDokumen73 halamanNew York Supreme Court: Appellate Division-Third DepartmentrkarlinBelum ada peringkat
- CHPE Petition For More DebtDokumen16 halamanCHPE Petition For More DebtrkarlinBelum ada peringkat
- Restaurant Guide To Reducing PlasticsDokumen50 halamanRestaurant Guide To Reducing PlasticsrkarlinBelum ada peringkat
- Fantasy Sports COA DecisionDokumen58 halamanFantasy Sports COA DecisionrkarlinBelum ada peringkat
- DECLETTERDokumen3 halamanDECLETTERrkarlinBelum ada peringkat
- Mayor Keeler Response To Tradebe CEO WeHearYou Essay (March 3 2022) (002..Dokumen2 halamanMayor Keeler Response To Tradebe CEO WeHearYou Essay (March 3 2022) (002..rkarlinBelum ada peringkat
- Solar Tax Assessment LawsuitDokumen89 halamanSolar Tax Assessment LawsuitrkarlinBelum ada peringkat
- Crypto Moratorium White PaperDokumen20 halamanCrypto Moratorium White PaperrkarlinBelum ada peringkat
- We Hear You, Cohoes, and We'd Like To Invest: by Victor Creixell de Vilallonga Global CEO, Tradebe Environmental ServicesDokumen3 halamanWe Hear You, Cohoes, and We'd Like To Invest: by Victor Creixell de Vilallonga Global CEO, Tradebe Environmental ServicesrkarlinBelum ada peringkat
- E2 PTAct 9 7 1 DirectionsDokumen4 halamanE2 PTAct 9 7 1 DirectionsEmzy SorianoBelum ada peringkat
- Iitk Syllabus PDFDokumen520 halamanIitk Syllabus PDFcombatps1Belum ada peringkat
- Abb Drives: User'S Manual Flashdrop Mfdt-01Dokumen62 halamanAbb Drives: User'S Manual Flashdrop Mfdt-01Сергей СалтыковBelum ada peringkat
- 1 Estafa - Arriola Vs PeopleDokumen11 halaman1 Estafa - Arriola Vs PeopleAtty Richard TenorioBelum ada peringkat
- Berry B Brey Part IDokumen49 halamanBerry B Brey Part Ikalpesh_chandakBelum ada peringkat
- Philippine Architecture, Film Industry EvolutionDokumen4 halamanPhilippine Architecture, Film Industry EvolutionCharly Mint Atamosa IsraelBelum ada peringkat
- Khadi Natural Company ProfileDokumen18 halamanKhadi Natural Company ProfileKleiton FontesBelum ada peringkat
- EWAIRDokumen1 halamanEWAIRKissy AndarzaBelum ada peringkat
- Mapping Groundwater Recharge Potential Using GIS-Based Evidential Belief Function ModelDokumen31 halamanMapping Groundwater Recharge Potential Using GIS-Based Evidential Belief Function Modeljorge “the jordovo” davidBelum ada peringkat
- Backup and Recovery ScenariosDokumen8 halamanBackup and Recovery ScenariosAmit JhaBelum ada peringkat
- Dwnload Full International Monetary Financial Economics 1st Edition Daniels Solutions Manual PDFDokumen36 halamanDwnload Full International Monetary Financial Economics 1st Edition Daniels Solutions Manual PDFelegiastepauleturc7u100% (16)
- Logistic Regression to Predict Airline Customer Satisfaction (LRCSDokumen20 halamanLogistic Regression to Predict Airline Customer Satisfaction (LRCSJenishBelum ada peringkat
- Com 0991Dokumen362 halamanCom 0991Facer DancerBelum ada peringkat
- POS CAL SF No4 B2 BCF H300x300 7mmweld R0 PDFDokumen23 halamanPOS CAL SF No4 B2 BCF H300x300 7mmweld R0 PDFNguyễn Duy QuangBelum ada peringkat
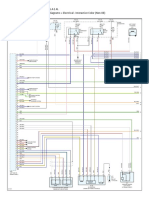
- Engine Controls (Powertrain Management) - ALLDATA RepairDokumen4 halamanEngine Controls (Powertrain Management) - ALLDATA Repairmemo velascoBelum ada peringkat
- Case Study - Soren ChemicalDokumen3 halamanCase Study - Soren ChemicalSallySakhvadzeBelum ada peringkat
- Dissolved Oxygen Primary Prod Activity1Dokumen7 halamanDissolved Oxygen Primary Prod Activity1api-235617848Belum ada peringkat
- Management Pack Guide For Print Server 2012 R2Dokumen42 halamanManagement Pack Guide For Print Server 2012 R2Quang VoBelum ada peringkat
- SDNY - Girl Scouts V Boy Scouts ComplaintDokumen50 halamanSDNY - Girl Scouts V Boy Scouts Complaintjan.wolfe5356Belum ada peringkat
- An Overview of National Ai Strategies and Policies © Oecd 2021Dokumen26 halamanAn Overview of National Ai Strategies and Policies © Oecd 2021wanyama DenisBelum ada peringkat
- Sapkale Sandspit 2020Dokumen5 halamanSapkale Sandspit 2020jbs_geoBelum ada peringkat
- Customer Satisfaction and Brand Loyalty in Big BasketDokumen73 halamanCustomer Satisfaction and Brand Loyalty in Big BasketUpadhayayAnkurBelum ada peringkat
- E-TON - Vector ST 250Dokumen87 halamanE-TON - Vector ST 250mariusgrosyBelum ada peringkat