Anda mungkin juga menyukai
- Canal IthDokumen4 halamanCanal IthSitthikorn StrikerrBelum ada peringkat
- BPPVDokumen10 halamanBPPVRizki MaulanaBelum ada peringkat
- Vertigo (An Evidence-Based Review) : Report of The Quality Practice Parameter: Therapies For Benign Paroxysmal PositionalDokumen10 halamanVertigo (An Evidence-Based Review) : Report of The Quality Practice Parameter: Therapies For Benign Paroxysmal PositionalfahlevyBelum ada peringkat
- Diagnosing and Treating BPPVDokumen22 halamanDiagnosing and Treating BPPVHeppyMeiBelum ada peringkat
- Diagnostic Value of Repeated Dix-Hallpike and Roll Maneuvers in Benign Paroxysmal Positional VertigoDokumen6 halamanDiagnostic Value of Repeated Dix-Hallpike and Roll Maneuvers in Benign Paroxysmal Positional VertigoShresthaBelum ada peringkat
- 2011-Visual Analog Scale To Assess Vertigo and Dizziness After Repositioning Maneuvers For Benign Paroxysmal Positional VertigoDokumen7 halaman2011-Visual Analog Scale To Assess Vertigo and Dizziness After Repositioning Maneuvers For Benign Paroxysmal Positional VertigoPingShun ChenBelum ada peringkat
- Vertigo (An Evidence-Based Review) : Report of The Quality Practice Parameter: Therapies For Benign Paroxysmal PositionalDokumen10 halamanVertigo (An Evidence-Based Review) : Report of The Quality Practice Parameter: Therapies For Benign Paroxysmal PositionalJulien CatherineBelum ada peringkat
- Gufoni ManeuvreDokumen6 halamanGufoni ManeuvreRudolfGerBelum ada peringkat
- Primary Total Shoulder Arthroplasty Performed Entirely Thru The Rotator Interval - Technique and Minimum Two-Year OutcomesDokumen10 halamanPrimary Total Shoulder Arthroplasty Performed Entirely Thru The Rotator Interval - Technique and Minimum Two-Year OutcomesmotohumeresBelum ada peringkat
- Comparison of Repositioning Maneuvers For Benign Paroxysmal Positional Vertigo of Posterior Semicircular Canal: Advantages of Hybrid ManeuverDokumen6 halamanComparison of Repositioning Maneuvers For Benign Paroxysmal Positional Vertigo of Posterior Semicircular Canal: Advantages of Hybrid ManeuverFayza RihastaraBelum ada peringkat
- Gufoni ManeuvreDokumen6 halamanGufoni ManeuvreRudolfGerBelum ada peringkat
- Screlosis Vestibular ReabilitationDokumen6 halamanScrelosis Vestibular Reabilitationandra_scooterBelum ada peringkat
- BPPV 2Dokumen10 halamanBPPV 2Dimas F. HidayatBelum ada peringkat
- Evidence-Based Review) : Report of The Quality Standards Subcommittee of The Practice Parameter: Therapies For Benign Paroxysmal Positional Vertigo (AnDokumen10 halamanEvidence-Based Review) : Report of The Quality Standards Subcommittee of The Practice Parameter: Therapies For Benign Paroxysmal Positional Vertigo (AnFajar MaskuriBelum ada peringkat
- The Immediate Effects of Lumbar Rotational Mobilization On Trunk Control and Gait Parameter in Patients With StrokeDokumen7 halamanThe Immediate Effects of Lumbar Rotational Mobilization On Trunk Control and Gait Parameter in Patients With Stroke林良駿Belum ada peringkat
- Articol Roberts OrlDokumen4 halamanArticol Roberts OrlSabina BădilăBelum ada peringkat
- Recovery Process of Gait Disturbance After Ventriculo-Peritoneal Shunt in Patients With Idiopathic Normal Pressure HydrocephalusDokumen6 halamanRecovery Process of Gait Disturbance After Ventriculo-Peritoneal Shunt in Patients With Idiopathic Normal Pressure HydrocephalusSARKAR JAVED AKHTARBelum ada peringkat
- Cytologic and Hematologic Tests Arterial Blood Gases: Medical Background: Chronic Restrictive Pulmonary DiseaseDokumen7 halamanCytologic and Hematologic Tests Arterial Blood Gases: Medical Background: Chronic Restrictive Pulmonary Diseasejoanna gurtizaBelum ada peringkat
- Difference in Balance Measures Between Patients With Chronic Ankle Instability and Patients After An Acute Ankle Inversion TraumaDokumen17 halamanDifference in Balance Measures Between Patients With Chronic Ankle Instability and Patients After An Acute Ankle Inversion TraumaAbu MishalBelum ada peringkat
- Jurnal Vertigo Post TraumaDokumen5 halamanJurnal Vertigo Post TraumaginapuspaBelum ada peringkat
- Vestibular Consequences in CIDokumen46 halamanVestibular Consequences in CIGhada WageihBelum ada peringkat
- tmp965D TMPDokumen16 halamantmp965D TMPFrontiersBelum ada peringkat
- Anaesthesia For Surgical Correction of Scoliosis With Spinal Cord Monitoring - A Case SeriesDokumen6 halamanAnaesthesia For Surgical Correction of Scoliosis With Spinal Cord Monitoring - A Case SeriesronnyBelum ada peringkat
- Effectiveness of The Canalith Repositioning Procedure in The Treatment of Benign Paroxysmal Positional VertigoDokumen11 halamanEffectiveness of The Canalith Repositioning Procedure in The Treatment of Benign Paroxysmal Positional VertigoNia UtariBelum ada peringkat
- All ReferanceDokumen34 halamanAll ReferanceKim AntelBelum ada peringkat
- Endoscopic Evaluation of Post-Fundoplication Anatomy: Esophagus (J Clarke and N Ahuja, Section Editors)Dokumen8 halamanEndoscopic Evaluation of Post-Fundoplication Anatomy: Esophagus (J Clarke and N Ahuja, Section Editors)Josseph EscobarBelum ada peringkat
- Long Term Impact Preoperator...Dokumen6 halamanLong Term Impact Preoperator...nistormaria492Belum ada peringkat
- Batuecas Caletrio2014Dokumen5 halamanBatuecas Caletrio2014Macarena Lucina FernándezBelum ada peringkat
- International Journal of Health Sciences and ResearchDokumen9 halamanInternational Journal of Health Sciences and ResearchLuqmanul HakimBelum ada peringkat
- Video Head Impulse Test: A Comparison and Analysis of Three Recording SystemsDokumen7 halamanVideo Head Impulse Test: A Comparison and Analysis of Three Recording SystemsankurBelum ada peringkat
- Effectiveness of Brandt Daroff, Semont and Epley ManeuversDokumen8 halamanEffectiveness of Brandt Daroff, Semont and Epley ManeuversNestri PrabandaniBelum ada peringkat
- Comparing A Non-Invasive Hemodynamic Monitor With Minimally Invasive Monitoring During Major Open Abdominal Surgery-2Dokumen6 halamanComparing A Non-Invasive Hemodynamic Monitor With Minimally Invasive Monitoring During Major Open Abdominal Surgery-2Nadhia KhairunnisaBelum ada peringkat
- Contin Educ Anaesth Crit Care Pain-2010-Agnew-33-7Dokumen5 halamanContin Educ Anaesth Crit Care Pain-2010-Agnew-33-7deadbysunriseeBelum ada peringkat
- The Caloric Test and The Video Head-Impulse Test in Patients With VertigoDokumen7 halamanThe Caloric Test and The Video Head-Impulse Test in Patients With VertigoDevi DaryaningsihBelum ada peringkat
- Design and Analysis of HSC-BPPV Diagnostic ManeuveDokumen11 halamanDesign and Analysis of HSC-BPPV Diagnostic ManeuveSelinay YAȘABelum ada peringkat
- Autologous Fat Transfer in Secondary Carpal Tunnel Release PDFDokumen7 halamanAutologous Fat Transfer in Secondary Carpal Tunnel Release PDFdrbantmBelum ada peringkat
- Treatment of Genu Recurvatum in Hemiparetic Adult Patients: A Systematic Literature ReviewDokumen11 halamanTreatment of Genu Recurvatum in Hemiparetic Adult Patients: A Systematic Literature ReviewRahmoucha HoukiBelum ada peringkat
- The Effects of The ReWalk™ Robotic System On Walking Capability in Paraplegic Spinal Cord Injury PatientsDokumen8 halamanThe Effects of The ReWalk™ Robotic System On Walking Capability in Paraplegic Spinal Cord Injury PatientsFrankChenBelum ada peringkat
- Vestibular Disorder Guide (updated 09/06Dokumen6 halamanVestibular Disorder Guide (updated 09/06Ecaterina ChiriacBelum ada peringkat
- Peroneal Reaction Times and Eversion Motor Response in Healthy and Unstable AnklesDokumen6 halamanPeroneal Reaction Times and Eversion Motor Response in Healthy and Unstable AnklesPatricia BortolottiBelum ada peringkat
- Dynamic MR Imaging of The Pelvic Floor: A Pictorial Review: © RSNA, 2009Dokumen42 halamanDynamic MR Imaging of The Pelvic Floor: A Pictorial Review: © RSNA, 2009Radio ResidentBelum ada peringkat
- Smith, 2002Dokumen5 halamanSmith, 2002CaioSelaimenBelum ada peringkat
- Ankle Sprain CPR For ManipulationDokumen13 halamanAnkle Sprain CPR For ManipulationChaim MalineBelum ada peringkat
- Tullberg-Manip Not Alter Sij Spine98Dokumen8 halamanTullberg-Manip Not Alter Sij Spine98Swapna HarnishBelum ada peringkat
- Principles of Ultrasonographic ImagingDokumen89 halamanPrinciples of Ultrasonographic ImagingDamian Ana MariaBelum ada peringkat
- The Effect of Early Canalith Repositioning On Benign Paroxysmal Positional Vertigo On RecurrenceDokumen5 halamanThe Effect of Early Canalith Repositioning On Benign Paroxysmal Positional Vertigo On RecurrencezanafiraBelum ada peringkat
- Low Dose Levobupivacaıne 0.5% With Fentanyl in Spinal Anaesthesia For Transurethral Resection of Prostate SurgeryDokumen6 halamanLow Dose Levobupivacaıne 0.5% With Fentanyl in Spinal Anaesthesia For Transurethral Resection of Prostate Surgeryblabarry1109Belum ada peringkat
- Vestibulo-Ocular Reflex and The Head Impulse Test: Reflexo Vestíbulo-Ocular e o Teste Do Impulso Da CabeçaDokumen3 halamanVestibulo-Ocular Reflex and The Head Impulse Test: Reflexo Vestíbulo-Ocular e o Teste Do Impulso Da CabeçaJimmy AlexanderBelum ada peringkat
- Effectiveness of The Canalith Repositioning Procedure in The Treatment of Benign Paroxysmal Positional VertigoDokumen11 halamanEffectiveness of The Canalith Repositioning Procedure in The Treatment of Benign Paroxysmal Positional VertigoFayza RihastaraBelum ada peringkat
- 1 s2.0 S1607551X09703614 MainDokumen8 halaman1 s2.0 S1607551X09703614 MainAchenk BarcelonistaBelum ada peringkat
- Effects of Forward Head Posture On Static and Dynamic Balance ControlDokumen4 halamanEffects of Forward Head Posture On Static and Dynamic Balance ControlShimaa HarounBelum ada peringkat
- t2 (2) FinalDokumen5 halamant2 (2) Finalkubra17.01.2000Belum ada peringkat
- PDF Passive Leg Raise PLR Test Stroke Volume Index SviDokumen3 halamanPDF Passive Leg Raise PLR Test Stroke Volume Index SviNama ManaBelum ada peringkat
- Basic and Advanced Operative Techniques in Orthognatic SurgeryDokumen23 halamanBasic and Advanced Operative Techniques in Orthognatic SurgeryAndrea Cárdenas SandovalBelum ada peringkat
- Chod Udar5Dokumen18 halamanChod Udar5Suman DeyBelum ada peringkat
- One Minute STST Vs 6MWT en EPOCDokumen10 halamanOne Minute STST Vs 6MWT en EPOCMaxi BoniniBelum ada peringkat
- Nau 24097Dokumen9 halamanNau 24097Anonymous ovTI4eBelum ada peringkat
- Disorders of the Patellofemoral Joint: Diagnosis and ManagementDari EverandDisorders of the Patellofemoral Joint: Diagnosis and ManagementBelum ada peringkat
- Atlas of High-Resolution Manometry, Impedance, and pH MonitoringDari EverandAtlas of High-Resolution Manometry, Impedance, and pH MonitoringBelum ada peringkat
- EVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYDari EverandEVALUATION OF THE INFLUENCE OF TWO DIFFERENT SYSTEMS OF ANALGESIA AND THE NASOGASTRIC TUBE ON THE INCIDENCE OF POSTOPERATIVE NAUSEA AND VOMITING IN CARDIAC SURGERYBelum ada peringkat
- GAGAL GINJAL KRONIS DAN INDIKASI DIALISISDokumen34 halamanGAGAL GINJAL KRONIS DAN INDIKASI DIALISISDjumadi AkbarBelum ada peringkat
- Principles of Diagnosis and Antimicrobial TherapyDokumen116 halamanPrinciples of Diagnosis and Antimicrobial TherapyD'nollas LadysBelum ada peringkat
- AcupunctureDokumen30 halamanAcupunctureDjumadi AkbarBelum ada peringkat
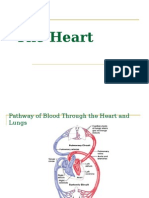
- HeartDokumen45 halamanHeartamelialyBelum ada peringkat
- Gangguan VisualDokumen17 halamanGangguan VisualDjumadi AkbarBelum ada peringkat
- Understanding Neuropati Perifer and Its CausesDokumen28 halamanUnderstanding Neuropati Perifer and Its CausesDjumadi AkbarBelum ada peringkat
- Kuliah 1. Effector Mechanism - Versi Ringkas 2013Dokumen55 halamanKuliah 1. Effector Mechanism - Versi Ringkas 2013Djumadi AkbarBelum ada peringkat
- The Digestive Apparatus UpperDokumen23 halamanThe Digestive Apparatus UpperDjumadi AkbarBelum ada peringkat
- Konsep Dasar Imunologi Sistem dan Kerja ImunDokumen43 halamanKonsep Dasar Imunologi Sistem dan Kerja ImunDjumadi Akbar100% (1)
- Chapter16 Immunological Tolerance (01) b6 m2Dokumen34 halamanChapter16 Immunological Tolerance (01) b6 m2Djumadi AkbarBelum ada peringkat
- Understanding Neuropati Perifer and Its CausesDokumen28 halamanUnderstanding Neuropati Perifer and Its CausesDjumadi AkbarBelum ada peringkat
- Konsep Dasar Imunologi Sistem dan Kerja ImunDokumen43 halamanKonsep Dasar Imunologi Sistem dan Kerja ImunDjumadi Akbar100% (1)
- Aspek Klinik Penyakit AutoimunDokumen46 halamanAspek Klinik Penyakit AutoimunDjumadi AkbarBelum ada peringkat
- Tiroid FK Ums 13Dokumen67 halamanTiroid FK Ums 13Djumadi AkbarBelum ada peringkat
- BrainstemDokumen47 halamanBrainstemReRe Pink100% (1)
- The Diagnosis and Treatment of The Cervical VertigoDokumen5 halamanThe Diagnosis and Treatment of The Cervical VertigoDjumadi AkbarBelum ada peringkat
- Tiroid FK Ums 13Dokumen67 halamanTiroid FK Ums 13Djumadi AkbarBelum ada peringkat
- AutoimunDokumen23 halamanAutoimunDjumadi AkbarBelum ada peringkat
- Patologi AnatomiDokumen9 halamanPatologi AnatomiDjumadi AkbarBelum ada peringkat
- CMPADokumen21 halamanCMPADjumadi AkbarBelum ada peringkat
- Blok 2Dokumen105 halamanBlok 2Djumadi AkbarBelum ada peringkat
- Understanding Cancer Immunology and Its Role in TreatmentDokumen40 halamanUnderstanding Cancer Immunology and Its Role in TreatmentDjumadi AkbarBelum ada peringkat
- Praktikum Protein: Fakultas Kedokteran UMS SurakartaDokumen10 halamanPraktikum Protein: Fakultas Kedokteran UMS SurakartaDjumadi AkbarBelum ada peringkat
- Chronic Tension Headache Mechanism and TreatmentDokumen5 halamanChronic Tension Headache Mechanism and TreatmentAchmad 'Eko' SBelum ada peringkat
- INFERTILITASDokumen29 halamanINFERTILITASDjumadi AkbarBelum ada peringkat
- Case Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDokumen5 halamanCase Report: Vertigo As A Predominant Manifestation of NeurosarcoidosisDjumadi AkbarBelum ada peringkat
- Congenital AbnormalitiesDokumen17 halamanCongenital AbnormalitiesDjumadi AkbarBelum ada peringkat
- Demographic Analysis of BPPV as a Common Health IssueDokumen4 halamanDemographic Analysis of BPPV as a Common Health IssueDjumadi AkbarBelum ada peringkat
- Binder 1Dokumen36 halamanBinder 1BobbyBelum ada peringkat
- Trafo 40 Mva PDFDokumen719 halamanTrafo 40 Mva PDFeug_manu8Belum ada peringkat
- BIS 14665 Part 2Dokumen6 halamanBIS 14665 Part 2Sunil ChadhaBelum ada peringkat
- Effects of Nimodipine, Vinpocetine and Their Combination On Isoproterenol-Induced Myocardial Infarction in RatsDokumen9 halamanEffects of Nimodipine, Vinpocetine and Their Combination On Isoproterenol-Induced Myocardial Infarction in RatsBilal AbbasBelum ada peringkat
- A-019730-1647416754604-137865-W.M.Supun Anjana DSADokumen175 halamanA-019730-1647416754604-137865-W.M.Supun Anjana DSADishan SanjayaBelum ada peringkat
- 10th Geometrical ConstructionDokumen2 halaman10th Geometrical Constructionapi-242227794100% (1)
- CB Climbing Bracket PERIDokumen52 halamanCB Climbing Bracket PERINathan FryerBelum ada peringkat
- Formation and Evolution of Planetary SystemsDokumen25 halamanFormation and Evolution of Planetary SystemsLovelyn Baltonado100% (2)
- Breathing AND Exchange of Gases MCQs PDFDokumen78 halamanBreathing AND Exchange of Gases MCQs PDFJatin SinglaBelum ada peringkat
- Unit 2Dokumen76 halamanUnit 2Mithila100% (1)
- Mapping Abap XML PDFDokumen88 halamanMapping Abap XML PDFassane2mcsBelum ada peringkat
- Triad Over Root Chords Companion PDF 2.1Dokumen18 halamanTriad Over Root Chords Companion PDF 2.1Vlado PetkovskiBelum ada peringkat
- Geometri Ruang File 1Dokumen4 halamanGeometri Ruang File 1Muhammad Isna SumaatmajaBelum ada peringkat
- What Is Radar and Its FunctionDokumen3 halamanWhat Is Radar and Its FunctionJean Maya DiscayaBelum ada peringkat
- BUS STAT Chapter-3 Freq DistributionDokumen5 halamanBUS STAT Chapter-3 Freq DistributionolmezestBelum ada peringkat
- Profit Signals How Evidence Based Decisions Power Six Sigma BreakthroughsDokumen262 halamanProfit Signals How Evidence Based Decisions Power Six Sigma BreakthroughsM. Daniel SloanBelum ada peringkat
- Experiment03 PCM-DecodingDokumen10 halamanExperiment03 PCM-DecodingMary Rose P Delos SantosBelum ada peringkat
- The Chemistry of Gemstone Colours 2016Dokumen1 halamanThe Chemistry of Gemstone Colours 2016Lukau João PedroBelum ada peringkat
- Driver MC34152Dokumen4 halamanDriver MC34152William RamírezBelum ada peringkat
- Assignment 2Dokumen6 halamanAssignment 2Umar ZahidBelum ada peringkat
- Lab Report Mass Spring System Omar Nizar2Dokumen31 halamanLab Report Mass Spring System Omar Nizar2Omar MustafaBelum ada peringkat
- 12 Translations PDFDokumen4 halaman12 Translations PDFTeo Lee Hong0% (1)
- Hikmayanto Hartawan PurchDokumen12 halamanHikmayanto Hartawan PurchelinBelum ada peringkat
- Managing Economies of Scale in Supply ChainsDokumen25 halamanManaging Economies of Scale in Supply ChainsWei JunBelum ada peringkat
- Reed - Camion - XT39R4 - 1003 - Technical Manual - Panel de Control PDFDokumen293 halamanReed - Camion - XT39R4 - 1003 - Technical Manual - Panel de Control PDFLuisEduardoHerreraCamargo100% (1)
- General Types of Intermolecular Forces 11-LDokumen33 halamanGeneral Types of Intermolecular Forces 11-LClarenz N. Turan100% (1)
- Model SRX-101A: Operation ManualDokumen31 halamanModel SRX-101A: Operation ManualSebastian SamolewskiBelum ada peringkat
- SP 5500 V5.1 1.0Dokumen17 halamanSP 5500 V5.1 1.0Rama Tenis CopecBelum ada peringkat
- SM Maintenance Instructions: Author: Lars Rydén, Konecranes AB, SwedenDokumen132 halamanSM Maintenance Instructions: Author: Lars Rydén, Konecranes AB, SwedenDan VekasiBelum ada peringkat