Anda mungkin juga menyukai
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Diff Betwn Inlay and Amalgam CavityDokumen7 halamanDiff Betwn Inlay and Amalgam CavityVinisha Vipin Sharma100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Criteria of SelectionDokumen12 halamanCriteria of SelectionVinisha Vipin SharmaBelum ada peringkat
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Non Surgical Management of Periapical Lesions Using Calcium HydroxideDokumen6 halamanNon Surgical Management of Periapical Lesions Using Calcium HydroxideVinisha Vipin SharmaBelum ada peringkat
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Challenges in Working Length DeterminationDokumen101 halamanChallenges in Working Length DeterminationVinisha Vipin SharmaBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Acupuncture in Dentistry PDFDokumen73 halamanAcupuncture in Dentistry PDFVinisha Vipin SharmaBelum ada peringkat
- Eaat 14 I 1 P 217Dokumen6 halamanEaat 14 I 1 P 217Vinisha Vipin SharmaBelum ada peringkat
- Mechanical Preparation Updated May2017 Prof Marco VersianiDokumen159 halamanMechanical Preparation Updated May2017 Prof Marco VersianiVinisha Vipin SharmaBelum ada peringkat
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Content ServerDokumen5 halamanContent ServerVinisha Vipin SharmaBelum ada peringkat
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Glide Path PreparationDokumen5 halamanGlide Path PreparationVinisha Vipin SharmaBelum ada peringkat
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Some Basics of LasersDokumen102 halamanSome Basics of LasersVinisha Vipin SharmaBelum ada peringkat
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Show TextDokumen1 halamanShow TextVinisha Vipin SharmaBelum ada peringkat
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Laser in Conservative Dentistry & EndodonticsDokumen75 halamanLaser in Conservative Dentistry & EndodonticsVinisha Vipin SharmaBelum ada peringkat
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Nanodentistry: New Buzz in Dentistry: Review ArticleDokumen5 halamanNanodentistry: New Buzz in Dentistry: Review ArticleVinisha Vipin SharmaBelum ada peringkat
- Practice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportDokumen5 halamanPractice: Radiographic Evidence of Postoperative Healing 12 Years Following Root Canal Treatment - A Case ReportVinisha Vipin SharmaBelum ada peringkat
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- EchsDokumen20 halamanEchsVinisha Vipin SharmaBelum ada peringkat
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Content ServerDokumen6 halamanContent ServerVinisha Vipin SharmaBelum ada peringkat
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Dentin HypersensitivityDokumen62 halamanDentin HypersensitivityVinisha Vipin Sharma100% (1)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
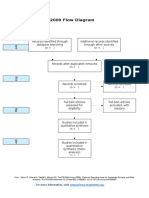
- PRISMA 2009 Flow Diagram: For More Information, VisitDokumen1 halamanPRISMA 2009 Flow Diagram: For More Information, VisitVinisha Vipin SharmaBelum ada peringkat
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Ceramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveDokumen5 halamanCeramic Restorations: Bonded Porcelain Veneers - Part 1: PerspectiveVinisha Vipin SharmaBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- PRISMA-P Statement - Moher Sys Rev Jan 2015Dokumen9 halamanPRISMA-P Statement - Moher Sys Rev Jan 2015Vinisha Vipin SharmaBelum ada peringkat
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- Pin Retained RestorationDokumen31 halamanPin Retained RestorationVinisha Vipin SharmaBelum ada peringkat
- Esthetic Alternatives To AmalgamDokumen15 halamanEsthetic Alternatives To AmalgamVinisha Vipin SharmaBelum ada peringkat
- Clarks Cavity PreparationDokumen10 halamanClarks Cavity PreparationVinisha Vipin SharmaBelum ada peringkat
- Welding Technology NotesDokumen89 halamanWelding Technology NotesSanjay JangraBelum ada peringkat
- Plant Cell WallDokumen2 halamanPlant Cell WallShiela BelandresBelum ada peringkat
- Astm G200 - 09Dokumen4 halamanAstm G200 - 09Sofia YuliBelum ada peringkat
- Ramabulana Et Al. 2021 MN and MetPA - Chemical Space of Four Momordica Plant SpeciesDokumen15 halamanRamabulana Et Al. 2021 MN and MetPA - Chemical Space of Four Momordica Plant SpeciesFernanda SantosBelum ada peringkat
- Jurnal International AmilumDokumen17 halamanJurnal International AmilumGhiyatsKalukuBelum ada peringkat
- Astm d1785Dokumen5 halamanAstm d1785Kehinde AdebayoBelum ada peringkat
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Applsci 08 01960 PDFDokumen17 halamanApplsci 08 01960 PDFphillynovitaBelum ada peringkat
- College of Nursing: Cebu Normal UniversityDokumen5 halamanCollege of Nursing: Cebu Normal UniversityChelsea WuBelum ada peringkat
- Kerosene As HealerDokumen17 halamanKerosene As HealerDuncan R Sickler100% (2)
- Rev004Dokumen3 halamanRev004Issam LahlouBelum ada peringkat
- Hot TappingDokumen21 halamanHot TappingnayakyaBelum ada peringkat
- Aeroquip HoseDokumen0 halamanAeroquip Hosegbm2246Belum ada peringkat
- Chemistry March 2008 EngDokumen7 halamanChemistry March 2008 EngPrasad C M0% (2)
- Astm A 240-18Dokumen12 halamanAstm A 240-18Giann' Andreh'xd100% (2)
- HDPE CatalogDokumen56 halamanHDPE CatalogSalwa AlsamnehBelum ada peringkat
- Planar MetalsDokumen11 halamanPlanar MetalsSilvano Prado0% (1)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Rna Qualitative TestsDokumen5 halamanRna Qualitative TestsPeter Paul RecaboBelum ada peringkat
- Grade 11: General Biology IDokumen38 halamanGrade 11: General Biology ITEOFILO GATDULABelum ada peringkat
- Carnauba-Super-Micropowder 2442 P 5: ApplicationDokumen1 halamanCarnauba-Super-Micropowder 2442 P 5: Application333cubi333Belum ada peringkat
- Hazen - William Coeficiente FBEDokumen10 halamanHazen - William Coeficiente FBEOrlandoBelum ada peringkat
- Catalogue 2011 DennerleDokumen64 halamanCatalogue 2011 DennerlebrusilicaBelum ada peringkat
- 70 Penetration Grade BitumenDokumen1 halaman70 Penetration Grade BitumenJohn SnowBelum ada peringkat
- Brochures WSM2-Y PDFDokumen16 halamanBrochures WSM2-Y PDFkunkzBelum ada peringkat
- 465Dokumen18 halaman465Mabel SanhuezaBelum ada peringkat
- Finals ReviewerDokumen5 halamanFinals ReviewerARIAR, Jyllianne Kyla C.Belum ada peringkat
- DNA-protein Interactions: Methods For Detection and AnalysisDokumen31 halamanDNA-protein Interactions: Methods For Detection and AnalysisAhsan Arshad BSIT-F16-LC-008Belum ada peringkat
- 3G Metric A4 Overview PDFDokumen8 halaman3G Metric A4 Overview PDFDiadam SharmaBelum ada peringkat
- Donaldon General Brochure WideDokumen20 halamanDonaldon General Brochure WidecivodulBelum ada peringkat
- Spe 180853 MSDokumen18 halamanSpe 180853 MSkerron_rekhaBelum ada peringkat
- Material Safety Data Sheet: Veolia Water Systems (Gulf) FZCDokumen2 halamanMaterial Safety Data Sheet: Veolia Water Systems (Gulf) FZCJHUPEL ABARIAL100% (1)
- Exposure: Poisoned Water, Corporate Greed, and One Lawyer's Twenty-Year Battle Against DuPontDari EverandExposure: Poisoned Water, Corporate Greed, and One Lawyer's Twenty-Year Battle Against DuPontPenilaian: 4.5 dari 5 bintang4.5/5 (18)
- Waste: One Woman’s Fight Against America’s Dirty SecretDari EverandWaste: One Woman’s Fight Against America’s Dirty SecretPenilaian: 5 dari 5 bintang5/5 (1)
- The Cyanide Canary: A True Story of InjusticeDari EverandThe Cyanide Canary: A True Story of InjusticePenilaian: 4 dari 5 bintang4/5 (52)
- Art of Commenting: How to Influence Environmental Decisionmaking With Effective Comments, The, 2d EditionDari EverandArt of Commenting: How to Influence Environmental Decisionmaking With Effective Comments, The, 2d EditionPenilaian: 3 dari 5 bintang3/5 (1)