Anda mungkin juga menyukai
- Molecular Diagnostics in Cytopathology: A Practical Handbook for the Practicing PathologistDari EverandMolecular Diagnostics in Cytopathology: A Practical Handbook for the Practicing PathologistSinchita Roy-ChowdhuriBelum ada peringkat
- Performance and Diagnostic Accuracy of A Urine-Based Human Papillomavirus Assay in A Referral PopulationDokumen7 halamanPerformance and Diagnostic Accuracy of A Urine-Based Human Papillomavirus Assay in A Referral PopulationJose de PapadopoulosBelum ada peringkat
- Arbyn2012IntJCancer AcceptedDokumen19 halamanArbyn2012IntJCancer AcceptedbehdadBelum ada peringkat
- Management of HPV Positive Cases After Screening: Alexandros I. DaponteDokumen37 halamanManagement of HPV Positive Cases After Screening: Alexandros I. DaponteHabtamu BiazinBelum ada peringkat
- Accuracy of Human Papillomavirus Testing On Self Collected Versus Clinician Collected Samples A Meta Analysis PDFDokumen12 halamanAccuracy of Human Papillomavirus Testing On Self Collected Versus Clinician Collected Samples A Meta Analysis PDFmarkinfonsecaBelum ada peringkat
- HPV E6E7 mRNA 1173 PatientDokumen9 halamanHPV E6E7 mRNA 1173 PatienthippopotamasBelum ada peringkat
- New England Journal Medicine: The ofDokumen10 halamanNew England Journal Medicine: The ofIrena McLaughlinBelum ada peringkat
- Experimental and Molecular Pathology: SciencedirectDokumen8 halamanExperimental and Molecular Pathology: SciencedirectrafaelaqBelum ada peringkat
- A Comparison of HPV DNA Testing and Liquid Based Cytology Over Three Rounds of Primary Cervical Screening Extended Follow Up in The ARTISTIC TrialDokumen8 halamanA Comparison of HPV DNA Testing and Liquid Based Cytology Over Three Rounds of Primary Cervical Screening Extended Follow Up in The ARTISTIC TrialJosé HidalgoBelum ada peringkat
- OvarianDokumen14 halamanOvarianherryBelum ada peringkat
- Detection of Precancerous Cervical Lesions Is Differential by Human Papillomavirus TypeDokumen6 halamanDetection of Precancerous Cervical Lesions Is Differential by Human Papillomavirus TypeChristopher Edwin100% (1)
- ACCP Cxca Screening 2011Dokumen8 halamanACCP Cxca Screening 2011Lizeth López LeónBelum ada peringkat
- OpophhoiDokumen7 halamanOpophhoiAnonymous i8CYD6bFrDBelum ada peringkat
- Arbyn2014 Metaanalisis VPH PDFDokumen12 halamanArbyn2014 Metaanalisis VPH PDFlunasanjuaneraBelum ada peringkat
- HPV DNA Testing in Cervical Cancer Screening: Results From Women in A High-Risk Province of Costa RicaDokumen7 halamanHPV DNA Testing in Cervical Cancer Screening: Results From Women in A High-Risk Province of Costa RicapathologyguruBelum ada peringkat
- Mustafa 2016Dokumen7 halamanMustafa 2016ejigsonBelum ada peringkat
- Ihk PapsmearDokumen8 halamanIhk PapsmearnovaBelum ada peringkat
- Performance of Commercial Reverse Line Blot Assays For Human Papillomavirus GenotypingDokumen6 halamanPerformance of Commercial Reverse Line Blot Assays For Human Papillomavirus GenotypingMuhammad Ricky RamadhianBelum ada peringkat
- Referencias de AMBUDokumen10 halamanReferencias de AMBUjosegarcia7Belum ada peringkat
- Breast CA ScreeningDokumen8 halamanBreast CA Screeningchristelm_1Belum ada peringkat
- Cytologic Patterns of Cervical Adenocarcinomas With Emphasis On Factors Associated With Underdiagnosis - Tumor DiathesisDokumen9 halamanCytologic Patterns of Cervical Adenocarcinomas With Emphasis On Factors Associated With Underdiagnosis - Tumor Diathesisnakemi111Belum ada peringkat
- HPV InfectionDokumen11 halamanHPV InfectionﺳﻮﺘﻴﺎﺳﻴﻪBelum ada peringkat
- DJP 367Dokumen12 halamanDJP 367Bibup GhaziyahBelum ada peringkat
- Plasma DNA Integrity Index in Breast Cancer PatientsDokumen19 halamanPlasma DNA Integrity Index in Breast Cancer PatientsSalwa Hassan TeamaBelum ada peringkat
- Cervical Cancer Screening With Human Papillomavirus DNA and Cytology in JapanDokumen7 halamanCervical Cancer Screening With Human Papillomavirus DNA and Cytology in Japandella kharisma putriBelum ada peringkat
- Oncology Letters 2014Dokumen9 halamanOncology Letters 2014anon_982215159Belum ada peringkat
- Gynecologic OncologyDokumen8 halamanGynecologic OncologyMariana HernandezBelum ada peringkat
- Research Article: The Bethesda System For Reporting Thyroid Cytopathology: A Cytohistological StudyDokumen8 halamanResearch Article: The Bethesda System For Reporting Thyroid Cytopathology: A Cytohistological StudyAbdullah KhalilBelum ada peringkat
- 2207OBG EvidenceDokumen2 halaman2207OBG EvidenceSandeep SharmaBelum ada peringkat
- Effective Screening23Dokumen10 halamanEffective Screening23ponekBelum ada peringkat
- Type-Specific Detection of 30 Oncogenic Human Papillomaviruses by Genotyping Both E6 and L1 GenesDokumen7 halamanType-Specific Detection of 30 Oncogenic Human Papillomaviruses by Genotyping Both E6 and L1 GenesNur Ghaliyah SandraBelum ada peringkat
- Miller Et Al, EEUU 2015Dokumen6 halamanMiller Et Al, EEUU 2015alexsr36Belum ada peringkat
- Baay Et Al-2004-International Journal of CancerDokumen4 halamanBaay Et Al-2004-International Journal of CancerGabriel ArnozoBelum ada peringkat
- HPV Types in 115789 HPV-pos Women - A Meta-Analysis From Cervical Infection To CancerDokumen11 halamanHPV Types in 115789 HPV-pos Women - A Meta-Analysis From Cervical Infection To CancerKen WayBelum ada peringkat
- Screen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource SettingsDokumen9 halamanScreen-and-Treat Approaches For Cervical Cancer Prevention in Low-Resource SettingsSaddam FuadBelum ada peringkat
- Plasma MesothelinDokumen7 halamanPlasma Mesothelinpaulo saBelum ada peringkat
- Anal Cytology 2019Dokumen7 halamanAnal Cytology 2019Cristina CostaBelum ada peringkat
- Breast Cancer Molecular Subtypes Respond Differently To Preoperative ChemotherapyDokumen8 halamanBreast Cancer Molecular Subtypes Respond Differently To Preoperative ChemotherapyPazitabknBelum ada peringkat
- Schiffman M Et Al. Gynecol Oncol. 2015.138 (3) .573-578Dokumen16 halamanSchiffman M Et Al. Gynecol Oncol. 2015.138 (3) .573-578eduardopr87Belum ada peringkat
- HPV16 Sublineage Associations With Histology-Specific Cancer Risk Using HPV Whole-Genome Sequences in 3200 WomenDokumen9 halamanHPV16 Sublineage Associations With Histology-Specific Cancer Risk Using HPV Whole-Genome Sequences in 3200 WomenQuyết Lê HữuBelum ada peringkat
- Assessment of Tumor Infiltrating Lymphocytes Using.12Dokumen9 halamanAssessment of Tumor Infiltrating Lymphocytes Using.12Muhammad Rifki100% (1)
- Exact ArticleDokumen6 halamanExact ArticleMuhammad WaqasBelum ada peringkat
- Breast Cancer Missed at Screening Hindsight or MiDokumen6 halamanBreast Cancer Missed at Screening Hindsight or MideaBelum ada peringkat
- Accuracy HPV Tests Urina Samples Meta AnalysisDokumen16 halamanAccuracy HPV Tests Urina Samples Meta AnalysisJuan Miguel GalarzaBelum ada peringkat
- HE4 and CA125 As A Diagnostic Test in Ovarian Cancer: Prospective Validation of The Risk of Ovarian Malignancy AlgorithmDokumen8 halamanHE4 and CA125 As A Diagnostic Test in Ovarian Cancer: Prospective Validation of The Risk of Ovarian Malignancy AlgorithmArifah GulamanisBelum ada peringkat
- HealthLinx Limited PaperDokumen10 halamanHealthLinx Limited PapermaikagmBelum ada peringkat
- Roe 2018Dokumen11 halamanRoe 2018mohamaed abbasBelum ada peringkat
- Articles: BackgroundDokumen12 halamanArticles: BackgroundMilan JovicBelum ada peringkat
- Uji Diagnostik Risk of Ovarian Malignancy Algorithm (ROMA) Dalam Menentukan Di RSUP Dr. Mohammad Hoesin PalembangDokumen6 halamanUji Diagnostik Risk of Ovarian Malignancy Algorithm (ROMA) Dalam Menentukan Di RSUP Dr. Mohammad Hoesin PalembangSarlitaIndahPermatasariBelum ada peringkat
- Jfac 142Dokumen25 halamanJfac 142Ana Paula Giolo FranzBelum ada peringkat
- HPV E6E7 mRNA Vs Pap SmearDokumen5 halamanHPV E6E7 mRNA Vs Pap SmearhippopotamasBelum ada peringkat
- Sabcs 2014 AllabstractsDokumen1.508 halamanSabcs 2014 Allabstractsrajesh4189Belum ada peringkat
- ACTN4-자궁경부암 관계 입증 논문-1Dokumen6 halamanACTN4-자궁경부암 관계 입증 논문-1김승훈(이과대학 화학)Belum ada peringkat
- Manuscript 4Dokumen4 halamanManuscript 4maryBelum ada peringkat
- Neutrophil To Lymphocyte Ratio (NLR) For Prediction of Distant Metastasis Free Survival (DMFS) in Early Breast CancerDokumen10 halamanNeutrophil To Lymphocyte Ratio (NLR) For Prediction of Distant Metastasis Free Survival (DMFS) in Early Breast CancerdrelvBelum ada peringkat
- Molecular Testing of Thyroid NodulesDokumen7 halamanMolecular Testing of Thyroid Nodulesayodeji78Belum ada peringkat
- NIH Public Access: Author ManuscriptDokumen18 halamanNIH Public Access: Author ManuscriptYosua_123Belum ada peringkat
- ARTICULODokumen8 halamanARTICULOCynthia Flora CruzBelum ada peringkat
- 1963 FullDokumen6 halaman1963 FullMichael StevenBelum ada peringkat
- Review ArticleDokumen16 halamanReview ArticleQudamah JasemBelum ada peringkat
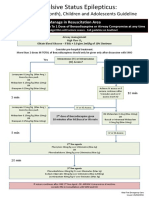
- Status Epilepticus A3v2Dokumen1 halamanStatus Epilepticus A3v2afalfitraBelum ada peringkat
- Experimental NeurologyDokumen12 halamanExperimental NeurologyafalfitraBelum ada peringkat
- EAbara How To Write A Case ReportDokumen19 halamanEAbara How To Write A Case ReportafalfitraBelum ada peringkat
- Interpretation of Arterial Blood Gases (ABGs)Dokumen6 halamanInterpretation of Arterial Blood Gases (ABGs)afalfitraBelum ada peringkat
- Research Thesis (P)Dokumen122 halamanResearch Thesis (P)dori sakBelum ada peringkat
- Treatment of HPVDokumen12 halamanTreatment of HPVsnow del carmenBelum ada peringkat
- (CPG) Philippine Guidelines On Periodic Health Examination: Pediatric ImmunizationDokumen171 halaman(CPG) Philippine Guidelines On Periodic Health Examination: Pediatric ImmunizationBianca Watanabe - RatillaBelum ada peringkat
- 1 s2.0 S0020748920302546 MainDokumen12 halaman1 s2.0 S0020748920302546 MainAnnisa Nur RamadhaniBelum ada peringkat
- Prevention Cervical Cancer4847Dokumen27 halamanPrevention Cervical Cancer4847Lalita Eka Pervita Sari100% (1)
- Clinical Investigation Cervix: y Z X K ( (Yy ZZ XX KK ( ( (Yyy ZZZ XXX XXXDokumen8 halamanClinical Investigation Cervix: y Z X K ( (Yy ZZ XX KK ( ( (Yyy ZZZ XXX XXXctuluBelum ada peringkat
- Cervical Cancer Thesis StatementDokumen6 halamanCervical Cancer Thesis StatementBecky Goins100% (2)
- Gynae-L - MukundaDokumen50 halamanGynae-L - MukundadocivirusBelum ada peringkat
- Topic 10 PDFDokumen28 halamanTopic 10 PDFAyad IdresBelum ada peringkat
- Obgy MCQDokumen20 halamanObgy MCQRajeswar KulanjiBelum ada peringkat
- Prevalence of Human Papillomavirus in Indonesia: A Population-Based Study in Three RegionsDokumen6 halamanPrevalence of Human Papillomavirus in Indonesia: A Population-Based Study in Three RegionsIlvita MayasariBelum ada peringkat
- Sgop CPGDokumen93 halamanSgop CPGjojolilimomo100% (2)
- HPV VaccineDokumen9 halamanHPV Vaccinearun babuBelum ada peringkat
- 2 Tumor Genital WanitaDokumen115 halaman2 Tumor Genital WanitaKhafidz Asy'ariBelum ada peringkat
- КРОК (англ) 2019Dokumen7 halamanКРОК (англ) 2019AimeeBelum ada peringkat
- Aquifer Case - Summary - FamilyMedicine17 - 55-YDokumen9 halamanAquifer Case - Summary - FamilyMedicine17 - 55-YHyunsoo EllisBelum ada peringkat
- Peerj 05 3910Dokumen13 halamanPeerj 05 3910Денис КрахоткинBelum ada peringkat
- Kanker Serviks ParitasDokumen7 halamanKanker Serviks Paritasveni safitri12Belum ada peringkat
- CVX Length SOGCDokumen14 halamanCVX Length SOGCBrendaBelum ada peringkat
- 1koss - Diagnostic - Cytology Its Origins and PrinciplesDokumen29 halaman1koss - Diagnostic - Cytology Its Origins and PrinciplesyoussefandabenBelum ada peringkat
- OB Gyne Clinical and Teaching CasesDokumen221 halamanOB Gyne Clinical and Teaching CaseszzBelum ada peringkat
- SPRITUAL Synopsis. FinalDokumen14 halamanSPRITUAL Synopsis. Finalsapna chauhanBelum ada peringkat
- Linus Pauling Institute Micronutrient Research For Optimum HealthDokumen9 halamanLinus Pauling Institute Micronutrient Research For Optimum HealthVivek KankipatiBelum ada peringkat
- Clinical Gynecologic OncologyDokumen809 halamanClinical Gynecologic Oncologyjhon heriansyahBelum ada peringkat
- Cellprep PaperDokumen8 halamanCellprep PapermuratcavasBelum ada peringkat
- Aristotle's EthicsDokumen30 halamanAristotle's EthicsJohn Michael BenderBelum ada peringkat
- Assignment Project ManagementDokumen15 halamanAssignment Project ManagementAhsanul Kabir SohanBelum ada peringkat
- Henrietta Lacks Reader's WorksheetDokumen5 halamanHenrietta Lacks Reader's WorksheetJonBelum ada peringkat
- Communicable and Non Communicable Diseases PDFDokumen96 halamanCommunicable and Non Communicable Diseases PDFhiabhijit2967% (3)