Anda mungkin juga menyukai
- PCV Lab-5 - HematologyDokumen4 halamanPCV Lab-5 - Hematologydhoha alawsiBelum ada peringkat
- Hematology Studies: Test: Total Hemoglobin (HGB or HB) CDokumen13 halamanHematology Studies: Test: Total Hemoglobin (HGB or HB) CSheena Arnoco ToraynoBelum ada peringkat
- Test: Total Hemoglobin (HGB or HB)Dokumen38 halamanTest: Total Hemoglobin (HGB or HB)Angiela JaurigueBelum ada peringkat
- Blood Grouping PDFDokumen23 halamanBlood Grouping PDFMaxamed Cali AtomBelum ada peringkat
- Hematocrit - StatPearls - NCBI BookshelfDokumen4 halamanHematocrit - StatPearls - NCBI BookshelfVincent ReyesBelum ada peringkat
- Hematocrit and Red Cell IndicesDokumen10 halamanHematocrit and Red Cell Indicespodcast gazalBelum ada peringkat
- Physiology Lab Report 2Dokumen27 halamanPhysiology Lab Report 2Chuan RuiBelum ada peringkat
- Red Blood Cell IndicesDokumen12 halamanRed Blood Cell IndicesKhalid AbdullahBelum ada peringkat
- Hematocrit: Method of MeasurementDokumen14 halamanHematocrit: Method of MeasurementRianaNurFatimahBelum ada peringkat
- Hematocrit (HCT) : June 2019Dokumen7 halamanHematocrit (HCT) : June 2019لطيفة نورBelum ada peringkat
- Hemoglobin Determination: Cyanmethemoglobin MethodDokumen31 halamanHemoglobin Determination: Cyanmethemoglobin Methodبراءة أحمد السلاماتBelum ada peringkat
- Fisio 7Dokumen11 halamanFisio 7anaBelum ada peringkat
- Hematocrit A Review of Different Analytical Methods PDFDokumen9 halamanHematocrit A Review of Different Analytical Methods PDFEsdras DountioBelum ada peringkat
- Red Blood Cell Indices: Presented By: Eusebio, Marielisa Mallari, Julianne Andre' ADokumen20 halamanRed Blood Cell Indices: Presented By: Eusebio, Marielisa Mallari, Julianne Andre' AJulianne MallariBelum ada peringkat
- Dr. Sanwar Agrawal MD Ekta Institute of Child Health Raipur: Published byDokumen26 halamanDr. Sanwar Agrawal MD Ekta Institute of Child Health Raipur: Published byRajarshi KumarBelum ada peringkat
- Laboratory Test InterpretationDokumen73 halamanLaboratory Test Interpretationjosieangel11Belum ada peringkat
- Hematology & UrinalysisDokumen77 halamanHematology & UrinalysismekuriawBelum ada peringkat
- Automated Hematology Cell CountersDokumen53 halamanAutomated Hematology Cell CountersFidaa Jaafrah100% (2)
- Hemoglobin Determination: Cyanmethemoglobin MethodDokumen32 halamanHemoglobin Determination: Cyanmethemoglobin MethodNasser DabiBelum ada peringkat
- Hematocrit (HCT) : Publication DetailsDokumen7 halamanHematocrit (HCT) : Publication DetailsPutri SyarifaniBelum ada peringkat
- Practical Clinical Hematology: Automated Hematology Cell CountersDokumen54 halamanPractical Clinical Hematology: Automated Hematology Cell CountersFidaa JaafrahBelum ada peringkat
- Hema Activity 3Dokumen5 halamanHema Activity 3Nico LokoBelum ada peringkat
- MICROHEMATOCRITDokumen19 halamanMICROHEMATOCRITNico LokoBelum ada peringkat
- Name: Gotoh, Aaron Tzergio C. DATE: 05/12/20 Erythrocyte Indices WorksheetDokumen3 halamanName: Gotoh, Aaron Tzergio C. DATE: 05/12/20 Erythrocyte Indices WorksheetMarie LlanesBelum ada peringkat
- Mean Corpuscular Hemoglobin ConcentrationDokumen2 halamanMean Corpuscular Hemoglobin ConcentrationMunish DograBelum ada peringkat
- Blood IndicesDokumen4 halamanBlood IndicesCharmaine RosalesBelum ada peringkat
- Hemoglobin and HematocritDokumen9 halamanHemoglobin and HematocritLovely B. AlipatBelum ada peringkat
- Clinical Haematology Lab. 1: Practical PhysiologyDokumen31 halamanClinical Haematology Lab. 1: Practical PhysiologyHameed SabahBelum ada peringkat
- CH 19 Case Study 1 Answer KeyDokumen3 halamanCH 19 Case Study 1 Answer KeyBryanBelum ada peringkat
- UPTODATE: Approach To The Adult With AnemiaDokumen8 halamanUPTODATE: Approach To The Adult With AnemiakimberlynBelum ada peringkat
- Evaluation of The Ruminant Complete Blood Dell CountDokumen26 halamanEvaluation of The Ruminant Complete Blood Dell CountDirección Científica Laboratorio VitalabBelum ada peringkat
- Relationship Between Hemoglobin and Platelet Count Among MBBS StudentsDokumen5 halamanRelationship Between Hemoglobin and Platelet Count Among MBBS StudentsIJAR JOURNALBelum ada peringkat
- Hematology Week 4 PDFDokumen9 halamanHematology Week 4 PDFKenj Yolleth IbañezBelum ada peringkat
- CBC InterpretationDokumen8 halamanCBC InterpretationAna Marie Reyes BansaleBelum ada peringkat
- Research Problem and SignificanceDokumen5 halamanResearch Problem and SignificancejvBelum ada peringkat
- MCHC - Red Cell Index or Quality Control Parameter?:, IncludingDokumen7 halamanMCHC - Red Cell Index or Quality Control Parameter?:, IncludingHerbanu PramonoBelum ada peringkat
- Decipher Your Labwork - CBC: Functional MedicineDari EverandDecipher Your Labwork - CBC: Functional MedicinePenilaian: 1 dari 5 bintang1/5 (1)
- Bio Vs PhytoDokumen23 halamanBio Vs PhytoNTA UGC-NETBelum ada peringkat
- MCHCDokumen4 halamanMCHCKryza Dale Bunado BaticanBelum ada peringkat
- FINAL Automated-HematologyDokumen67 halamanFINAL Automated-HematologyDineshprakash GovindhrajBelum ada peringkat
- Schalms Veterinary Hematology Clasificacion de Las Anemias 126563210056 127034822226Dokumen11 halamanSchalms Veterinary Hematology Clasificacion de Las Anemias 126563210056 127034822226Saica MédicalesBelum ada peringkat
- Solomon 2004Dokumen9 halamanSolomon 2004veaceslav coscodanBelum ada peringkat
- Hema Lab MidtermDokumen130 halamanHema Lab MidtermTrangia, SharmaineBelum ada peringkat
- HematologyDokumen34 halamanHematologyAnne Angue GonzalesBelum ada peringkat
- 4 Basic Hematological TechniquesDokumen11 halaman4 Basic Hematological TechniquesiamhannakarimBelum ada peringkat
- p1541 - Vol 84 - 9 PDFDokumen5 halamanp1541 - Vol 84 - 9 PDFmresearchBelum ada peringkat
- The Complete Blood Cell Count A PowerfulDokumen16 halamanThe Complete Blood Cell Count A PowerfulGabriele VitorBelum ada peringkat
- White Blood Cells Red Blood Cells Platelets: Complete Blood Count (CBC)Dokumen11 halamanWhite Blood Cells Red Blood Cells Platelets: Complete Blood Count (CBC)bsonBelum ada peringkat
- Diagnostic Approach To Anemia in Adults - UpToDateDokumen76 halamanDiagnostic Approach To Anemia in Adults - UpToDateanweridrisejazBelum ada peringkat
- Differences in Changes of Hemoglobin Between 6-12 Hours and 12-14 Hours After TransfusionDokumen4 halamanDifferences in Changes of Hemoglobin Between 6-12 Hours and 12-14 Hours After TransfusionAngel 冯晓君Belum ada peringkat
- CBC Test - What Is The Normal Range, What Do Abnormal Levels IndicateDokumen8 halamanCBC Test - What Is The Normal Range, What Do Abnormal Levels IndicateRedcliffe LabsBelum ada peringkat
- Case 1: 25 Yr Old Patient With History of FatigueDokumen79 halamanCase 1: 25 Yr Old Patient With History of FatigueMira WryczaBelum ada peringkat
- University of Hargeisa: Introduction of Hematology IDokumen19 halamanUniversity of Hargeisa: Introduction of Hematology IIsmo GurdeeyeBelum ada peringkat
- 2814 1Dokumen73 halaman2814 1Trangia, SharmaineBelum ada peringkat
- Anemia Diagnosis, Classification, and Monitoring Using Cell-Dyn Technology Reviewed For The New MillenniumDokumen16 halamanAnemia Diagnosis, Classification, and Monitoring Using Cell-Dyn Technology Reviewed For The New MillenniumNeveen_Hussein_1880Belum ada peringkat
- Bloodand Blood Product Admin STEGH2008Dokumen80 halamanBloodand Blood Product Admin STEGH2008Eric De TorresBelum ada peringkat
- LabDokumen28 halamanLabChamCham AquinoBelum ada peringkat
- Haematology 2 ManualDokumen26 halamanHaematology 2 Manualhayamitib11Belum ada peringkat
- What Is The Complete Blood Count Test (CBC) ?: White Blood Cells Red Blood Cells PlateletsDokumen4 halamanWhat Is The Complete Blood Count Test (CBC) ?: White Blood Cells Red Blood Cells PlateletsSheryl Ann Celis BacaniBelum ada peringkat
- 2014.PanduanLayananKlinisDokterSpesialisDermatologiDanVenereologi DR - RetnoDokumen22 halaman2014.PanduanLayananKlinisDokterSpesialisDermatologiDanVenereologi DR - RetnoBoby ShéBelum ada peringkat
- 2014.PanduanLayananKlinisDokterSpesialisDermatologiDanVenereologi DR - Retno PDFDokumen47 halaman2014.PanduanLayananKlinisDokterSpesialisDermatologiDanVenereologi DR - Retno PDFBoby ShéBelum ada peringkat
- 2014.panduan Layanan Klinis Dokter Spesialis Dermatologi Dan Venereologi Dr. RetnoDokumen47 halaman2014.panduan Layanan Klinis Dokter Spesialis Dermatologi Dan Venereologi Dr. RetnoBoby ShéBelum ada peringkat
- TpiDokumen72 halamanTpiBoby Shé0% (1)
- GINA Under5 Pocket 20091 1Dokumen0 halamanGINA Under5 Pocket 20091 1Boby ShéBelum ada peringkat
- Molecule Reaction Type / / Coenzymes: Figure 1: Schematic Drawing of The Citric Acid CycleDokumen1 halamanMolecule Reaction Type / / Coenzymes: Figure 1: Schematic Drawing of The Citric Acid CycleBoby ShéBelum ada peringkat
- This Is An Electronic Report & Not: To Be Used For Any Legal PurposesDokumen1 halamanThis Is An Electronic Report & Not: To Be Used For Any Legal PurposesMinhas ArshadBelum ada peringkat
- ChevronLab 1499245 3490149 171019110543 PDFDokumen1 halamanChevronLab 1499245 3490149 171019110543 PDFShoaib hossainBelum ada peringkat
- Sacchi Dan andDokumen2 halamanSacchi Dan andVINAYBelum ada peringkat
- Pathology & Clinical Laboratory (M) SDN - BHD: Scan QR For VerificationDokumen1 halamanPathology & Clinical Laboratory (M) SDN - BHD: Scan QR For VerificationAzhar SabriBelum ada peringkat
- IBN SINA PackageDokumen25 halamanIBN SINA PackageImtiaz BejoyBelum ada peringkat
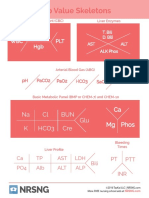
- Lab Value Skeletons: Ca MG Phos Na CL BUN K Hco3 Cre GluDokumen1 halamanLab Value Skeletons: Ca MG Phos Na CL BUN K Hco3 Cre GluGloryJaneBelum ada peringkat
- Profil Penderita CBDDokumen12 halamanProfil Penderita CBDVandra PrinosaBelum ada peringkat
- National Cancer Institute 268/1 Rama 6 Road Thung Phaya Thai, Ratchathewi, Bangkok 10400 Tel. 02-202-6800, 02-202-6888Dokumen2 halamanNational Cancer Institute 268/1 Rama 6 Road Thung Phaya Thai, Ratchathewi, Bangkok 10400 Tel. 02-202-6800, 02-202-6888Choo HokiertiBelum ada peringkat
- Conversion Table For Blood Glucose MonitoringDokumen1 halamanConversion Table For Blood Glucose MonitoringCamillus SamuilBelum ada peringkat
- SC003 1 Order of Draw WebsiteDokumen3 halamanSC003 1 Order of Draw WebsitemariamBelum ada peringkat
- Nilai Normal AbnormalDokumen4 halamanNilai Normal Abnormalaldy umasangadjiBelum ada peringkat
- Lab Result Kiran Farebrother VDRLDokumen1 halamanLab Result Kiran Farebrother VDRLMazterMaztermaztermazter MaztermaztermazterYandeBelum ada peringkat
- Tolentino, Ricardo Agustin 2284019178Dokumen1 halamanTolentino, Ricardo Agustin 2284019178Brielle DyBelum ada peringkat
- Hasil Lab An. CDokumen2 halamanHasil Lab An. CDENNYBelum ada peringkat
- Centrifuge Motor Rebuilding Catalog 2011Dokumen15 halamanCentrifuge Motor Rebuilding Catalog 2011Shan AhmadBelum ada peringkat
- Mindray Coagulation Reagent PT, APTT, FIB, TT BrochureDokumen1 halamanMindray Coagulation Reagent PT, APTT, FIB, TT BrochureAIIBelum ada peringkat
- Laporan Kinerja Lab Per Pasien Pemeriksaan 2022-07-24 S - D 2022-07-24Dokumen48 halamanLaporan Kinerja Lab Per Pasien Pemeriksaan 2022-07-24 S - D 2022-07-24LaboratoriumBelum ada peringkat
- Eurton Electric Co., Inc.: AbbottDokumen16 halamanEurton Electric Co., Inc.: Abbottjose navaBelum ada peringkat
- Biochemistry Report: Test Is Carried Out by Dimension EXL 200Dokumen1 halamanBiochemistry Report: Test Is Carried Out by Dimension EXL 200KH. A. H. M. SAYEF 1706024Belum ada peringkat
- 25 Yr(s) Sex:Male 13190414867 26 Apr 2019 15:15 26 Apr 2019 18:48Dokumen1 halaman25 Yr(s) Sex:Male 13190414867 26 Apr 2019 15:15 26 Apr 2019 18:48arpan mukherjeeBelum ada peringkat
- Keterampilan Pemeriksaan Hapusan Darah Terapi: Pembimbing: Dr. Herwindo Pudjo Brahmantyo, SP - PDDokumen29 halamanKeterampilan Pemeriksaan Hapusan Darah Terapi: Pembimbing: Dr. Herwindo Pudjo Brahmantyo, SP - PDTania Krisna PutriBelum ada peringkat
- Nipro Trueresult ManualDokumen82 halamanNipro Trueresult Manualfeliperm41Belum ada peringkat
- Department of Pathology and Laboratory Medicine: Test Result Units Reference RangeDokumen5 halamanDepartment of Pathology and Laboratory Medicine: Test Result Units Reference Rangecileen antabliBelum ada peringkat
- Bhagwanbloodreport - 23 - 888071pdf (2) - 230719 - 065846Dokumen1 halamanBhagwanbloodreport - 23 - 888071pdf (2) - 230719 - 065846Ajay SinghBelum ada peringkat
- Client Package Manual (Magsaysay - WestfalLarsen Management AS)Dokumen8 halamanClient Package Manual (Magsaysay - WestfalLarsen Management AS)Shalinur GonzalesBelum ada peringkat
- Grafik QC Hematologi 2023 BaruDokumen125 halamanGrafik QC Hematologi 2023 BaruSyifa nurfitriBelum ada peringkat
- Saniya Fathima (7G28Jy) :::: Patient Age / Sex 26 Y / Female BranchDokumen3 halamanSaniya Fathima (7G28Jy) :::: Patient Age / Sex 26 Y / Female BranchShah FaisalBelum ada peringkat
- Test Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Dokumen7 halamanTest Name Value Unit Biological Ref Interval Biochemistry Liver Function Test (LFT)Himanshu GarkhelBelum ada peringkat
- L96 - M/S Om Sai Path Lab Chiriyatand Khas Mahal More Patna BIHAR Mobile No:9334498936Dokumen2 halamanL96 - M/S Om Sai Path Lab Chiriyatand Khas Mahal More Patna BIHAR Mobile No:9334498936sunny SINGHBelum ada peringkat
- Lal Pathlabs ReportDokumen2 halamanLal Pathlabs ReportindianroadromeoBelum ada peringkat