Anda mungkin juga menyukai
- Automated Estimation of The Number of Contributors in AutosomalDokumen2 halamanAutomated Estimation of The Number of Contributors in AutosomalRuben MonroyBelum ada peringkat
- The American College of Surgeons Responds To COVID-19Dokumen7 halamanThe American College of Surgeons Responds To COVID-19Ruben MonroyBelum ada peringkat
- Outcomes of Patients With COVID-19 in The Intensive Care Unit in MexicoDokumen5 halamanOutcomes of Patients With COVID-19 in The Intensive Care Unit in MexicoRuben MonroyBelum ada peringkat
- A Rapid Molecular Diagnosis of CutaneousDokumen4 halamanA Rapid Molecular Diagnosis of CutaneousRuben MonroyBelum ada peringkat
- Comparative Study On The Effectiveness of DifferentDokumen8 halamanComparative Study On The Effectiveness of DifferentRuben MonroyBelum ada peringkat
- Research Response To COVID-19Dokumen30 halamanResearch Response To COVID-19Ruben MonroyBelum ada peringkat
- Incidence Rates of Hospitalization and Death From COVID-19Dokumen16 halamanIncidence Rates of Hospitalization and Death From COVID-19Ruben MonroyBelum ada peringkat
- The Importance of The Multidisciplinary ApproachDokumen5 halamanThe Importance of The Multidisciplinary ApproachRuben MonroyBelum ada peringkat
- Extremely Low Prevalence of Asymptomatic COVID-19Dokumen4 halamanExtremely Low Prevalence of Asymptomatic COVID-19Ruben MonroyBelum ada peringkat
- Agent-Based Mathematical ModelingDokumen11 halamanAgent-Based Mathematical ModelingRuben MonroyBelum ada peringkat
- Regulation of Intrinsic Apoptosis in CycloheximideDokumen10 halamanRegulation of Intrinsic Apoptosis in CycloheximideRuben MonroyBelum ada peringkat
- Characterization of Asymptomatic PlasmodiumDokumen5 halamanCharacterization of Asymptomatic PlasmodiumRuben MonroyBelum ada peringkat
- Nestedness Patterns of Sand FlyDokumen7 halamanNestedness Patterns of Sand FlyRuben MonroyBelum ada peringkat
- Phenology and Host PreferencesDokumen6 halamanPhenology and Host PreferencesRuben MonroyBelum ada peringkat
- Evidence For AnthropophilyDokumen7 halamanEvidence For AnthropophilyRuben MonroyBelum ada peringkat
- The 18Th Congress of The Society of Hair Testing (Soht) in GenevaDokumen1 halamanThe 18Th Congress of The Society of Hair Testing (Soht) in GenevaRuben MonroyBelum ada peringkat
- Identification of TgAtg8-TgAtg3 InteractionDokumen7 halamanIdentification of TgAtg8-TgAtg3 InteractionRuben MonroyBelum ada peringkat
- Breeding Habitat Preference of Preimaginal BlackDokumen7 halamanBreeding Habitat Preference of Preimaginal BlackRuben MonroyBelum ada peringkat
- 2 AminoethoxyDokumen8 halaman2 AminoethoxyRuben MonroyBelum ada peringkat
- An Epidemiological Study of DengueDokumen7 halamanAn Epidemiological Study of DengueRuben MonroyBelum ada peringkat
- Miranda LundyDokumen6 halamanMiranda LundyRuben MonroyBelum ada peringkat
- Serological Survey of Bovine BrucellosisDokumen8 halamanSerological Survey of Bovine BrucellosisRuben MonroyBelum ada peringkat
- 25B-NBOMe and Its Precursor 2C-B Modern Trends and HiddenDokumen11 halaman25B-NBOMe and Its Precursor 2C-B Modern Trends and HiddenRuben MonroyBelum ada peringkat
- Development and Application of GC-MSDokumen8 halamanDevelopment and Application of GC-MSRuben MonroyBelum ada peringkat
- Hair Decontamination ProcedureDokumen12 halamanHair Decontamination ProcedureRuben MonroyBelum ada peringkat
- International Renal-Cell-Cancer Study. Vi. The Role of Medical and Family HistoryDokumen4 halamanInternational Renal-Cell-Cancer Study. Vi. The Role of Medical and Family HistoryRuben MonroyBelum ada peringkat
- 2 AminoethoxyDokumen8 halaman2 AminoethoxyRuben MonroyBelum ada peringkat
- Applying Diagnostic Criteria For Type 1 Von Willebrand Disease To A Pediatric PopulationDokumen6 halamanApplying Diagnostic Criteria For Type 1 Von Willebrand Disease To A Pediatric PopulationRuben MonroyBelum ada peringkat
- Introgression and Dispersal Among Spotted OwlDokumen11 halamanIntrogression and Dispersal Among Spotted OwlRuben MonroyBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Mono 114Dokumen511 halamanMono 114Jose Angel AbadíaBelum ada peringkat
- Biochem-Rebecca NEET Recall 2020 PDFDokumen21 halamanBiochem-Rebecca NEET Recall 2020 PDFNaazneen MohammedBelum ada peringkat
- Caribbean Society and Culture - EssayDokumen1 halamanCaribbean Society and Culture - EssaySM WaterBelum ada peringkat
- Cast Metal Inlays - OnlaysDokumen7 halamanCast Metal Inlays - Onlaysdent in dentistBelum ada peringkat
- Physical Assesment For ChickenpoxDokumen6 halamanPhysical Assesment For ChickenpoxMary Gem Galvan FesalbonBelum ada peringkat
- Three in A Row A Case Series of Cervical TuberculosisDokumen6 halamanThree in A Row A Case Series of Cervical TuberculosisJonelle baloloyBelum ada peringkat
- Knowledge, Attitudes and Practices of Caregivers in Relation To Oral Health of Preschool ChildrenDokumen6 halamanKnowledge, Attitudes and Practices of Caregivers in Relation To Oral Health of Preschool ChildrenYayas Qori AwwaliBelum ada peringkat
- Keever FamilyDokumen2 halamanKeever FamilymarylcookpubliclibraBelum ada peringkat
- Phimosis 5 PDFDokumen4 halamanPhimosis 5 PDFNurul YaqinBelum ada peringkat
- PG 2nd Re Matching ResultDokumen31 halamanPG 2nd Re Matching ResultBinayak UpadhyayaBelum ada peringkat
- Closure of Midline Diastema by Multidisciplinary Approach - A Case ReportDokumen5 halamanClosure of Midline Diastema by Multidisciplinary Approach - A Case ReportAnonymous izrFWiQBelum ada peringkat
- Slipped Disc Syndrome ExplainedDokumen9 halamanSlipped Disc Syndrome ExplainedAndrei MarinBelum ada peringkat
- Safe IV CannulationDokumen32 halamanSafe IV Cannulationanon_281166672Belum ada peringkat
- PleuraFlow Brochure ML004 I FINALDokumen4 halamanPleuraFlow Brochure ML004 I FINALxergiogcBelum ada peringkat
- Cutting, Clamping and Retracting Surgical InstrumentsDokumen77 halamanCutting, Clamping and Retracting Surgical InstrumentsAndrea Pugh0% (1)
- Bogduk - Pain DefinitionDokumen3 halamanBogduk - Pain DefinitiontapiocadudeBelum ada peringkat
- 1 5053054235202027721Dokumen175 halaman1 5053054235202027721andifa aziz satriawanBelum ada peringkat
- Torts Cases: I. Fe Cayao vs. Ramolete FactsDokumen16 halamanTorts Cases: I. Fe Cayao vs. Ramolete FactsJana GonzalezBelum ada peringkat
- Pharmacy Law Name - 2 Year Pharmacy TechnicianDokumen9 halamanPharmacy Law Name - 2 Year Pharmacy TechnicianridaBelum ada peringkat
- Cdbb-Guide Vocal-Techniques EN PDFDokumen17 halamanCdbb-Guide Vocal-Techniques EN PDFrox100% (1)
- CASE STUDY PPT of PolyhydramniosDokumen59 halamanCASE STUDY PPT of PolyhydramniosAliza Savarez58% (12)
- Nursing Fundamental Q&ADokumen26 halamanNursing Fundamental Q&ALinjumol T GBelum ada peringkat
- Alternative Herbal Medicines and Therapies ExplainedDokumen25 halamanAlternative Herbal Medicines and Therapies ExplainedJuami OsmeñaBelum ada peringkat
- Drug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, VecuroniumDokumen12 halamanDrug Study Amphotericin B, Meropenem, Furosemide, Ciprofloxacin, Pentoxifylline, Pip-Tazo, Midazolam, Vecuroniumpaupaulala100% (4)
- ETHICS & CommunityDokumen47 halamanETHICS & CommunityShuaib AhmedBelum ada peringkat
- GPAT Question Papers, Drug Inspector, DCO Pharmacist ExamsDokumen9 halamanGPAT Question Papers, Drug Inspector, DCO Pharmacist ExamsSwaroopSinghJakharBelum ada peringkat
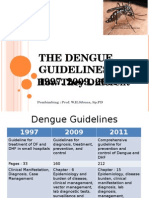
- Guideline Evolution for Diagnosis and Management of DengueDokumen35 halamanGuideline Evolution for Diagnosis and Management of DengueFrinciaBelum ada peringkat
- D S T E I B D B V: Esirable Pecifications For Otal Rror, Mprecision, and Ias, Erived From Iologic AriationDokumen14 halamanD S T E I B D B V: Esirable Pecifications For Otal Rror, Mprecision, and Ias, Erived From Iologic Ariationlaboratorium rsud jatipadangBelum ada peringkat
- Breech Presentation - PPT (Read-Only)Dokumen5 halamanBreech Presentation - PPT (Read-Only)Nestor SantiagoBelum ada peringkat
- Task Risk Assessment For QA QC and InspectionDokumen1 halamanTask Risk Assessment For QA QC and InspectionDhanasekar BalaBelum ada peringkat