Anda mungkin juga menyukai
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Biblical Names in AmharicDokumen275 halamanBiblical Names in AmharicMichal wojcik75% (8)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Aphrodisiac Plants List Used in Unani Medicine (Abstract)Dokumen4 halamanAphrodisiac Plants List Used in Unani Medicine (Abstract)Michal wojcikBelum ada peringkat
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Doctrine of MayaDokumen164 halamanThe Doctrine of Mayasukubh100% (1)
- Normal & Abnormal GaitDokumen29 halamanNormal & Abnormal GaitVidhya anand MBelum ada peringkat
- Nakshatras - The Real Secrets of Vedic AstrologyDokumen39 halamanNakshatras - The Real Secrets of Vedic AstrologyMichal wojcik100% (4)
- Glen Keane NotesDokumen22 halamanGlen Keane NotesLilian Yuri Ishida100% (2)
- Amarigna and Tigrigna Qal Hieroglyphs PDFDokumen84 halamanAmarigna and Tigrigna Qal Hieroglyphs PDFMichal wojcik100% (1)
- Occupational AnalysisDokumen19 halamanOccupational Analysisapi-238453631Belum ada peringkat
- Chapter 5: AerobicsDokumen12 halamanChapter 5: AerobicsMa Therese A CaycoBelum ada peringkat
- Medicine of The Prophet - Bhikha & DokraDokumen202 halamanMedicine of The Prophet - Bhikha & DokraMichal wojcik100% (9)
- The Perfect Exercise - Ba Gua Circle Walking Nei GungDokumen6 halamanThe Perfect Exercise - Ba Gua Circle Walking Nei GungLaron ClarkBelum ada peringkat
- Chukka Full Patterns FreeDokumen71 halamanChukka Full Patterns FreeSergey CheBelum ada peringkat
- Being Young & Muslim ..In Global South & North - L. Herrera & A. Bayat PDFDokumen445 halamanBeing Young & Muslim ..In Global South & North - L. Herrera & A. Bayat PDFMichal wojcik50% (2)
- Strategy A Short Guide (23p) Martin Van CreveldDokumen23 halamanStrategy A Short Guide (23p) Martin Van CreveldMichal wojcikBelum ada peringkat
- Izibongo: John MuafangejoDokumen16 halamanIzibongo: John MuafangejoMichal wojcikBelum ada peringkat
- Physical Education: Quarter 2 - Module 1: Walking and Running ProgramDokumen34 halamanPhysical Education: Quarter 2 - Module 1: Walking and Running ProgramNiko Igie Albino Pujeda63% (8)
- Abdominaux Arretez Le MassacreDokumen688 halamanAbdominaux Arretez Le MassacreMichal wojcikBelum ada peringkat
- Izibongo 02Dokumen12 halamanIzibongo 02Michal wojcikBelum ada peringkat
- Thayumanavar - The Silent Sage - A Short BiographyDokumen27 halamanThayumanavar - The Silent Sage - A Short BiographyMichal wojcikBelum ada peringkat
- Urban Design TheoriesDokumen20 halamanUrban Design TheoriesBich Ngoc LeBelum ada peringkat
- Are Pedestrians Invisible in The Planning Process? Copenhagen As A Case StudyDokumen8 halamanAre Pedestrians Invisible in The Planning Process? Copenhagen As A Case StudyDaisyBelum ada peringkat
- 4188843Dokumen10 halaman4188843midahrazalBelum ada peringkat
- BeginningofbootymanualDokumen17 halamanBeginningofbootymanualapi-31163190350% (2)
- Date and Time Objectives Learning Contents Strategies Target Population Resources Evaluation OutcomeDokumen8 halamanDate and Time Objectives Learning Contents Strategies Target Population Resources Evaluation OutcometrizzlecBelum ada peringkat
- 2023 D2 FP Footwear Spring CatalogDokumen31 halaman2023 D2 FP Footwear Spring CatalogOni K.Belum ada peringkat
- Ebn 1Dokumen14 halamanEbn 1Faisal HarisBelum ada peringkat
- Footwear Industry in IndiaDokumen26 halamanFootwear Industry in IndiaASHA05Belum ada peringkat
- Assisting A Patient With Ambulation Using A Cane: Page 1/2Dokumen2 halamanAssisting A Patient With Ambulation Using A Cane: Page 1/2Mac Cristian A. CaraganBelum ada peringkat
- Kisi Soal AKM BING Kls 7 Genap2020 - TriDokumen3 halamanKisi Soal AKM BING Kls 7 Genap2020 - TriTri MacoaloBelum ada peringkat
- Gait & Posture: Kristen L. Hollands, Trudy A. Pelton, Sarah F. Tyson, Mark A. Hollands, Paulette M. Van VlietDokumen11 halamanGait & Posture: Kristen L. Hollands, Trudy A. Pelton, Sarah F. Tyson, Mark A. Hollands, Paulette M. Van VlietMariaBelum ada peringkat
- Prosthetic Knee SystemsDokumen2 halamanProsthetic Knee SystemshppresarioBelum ada peringkat
- Atestat EnglezaDokumen34 halamanAtestat EnglezaMladinTiberiuBelum ada peringkat
- Exercise PDF FinalDokumen43 halamanExercise PDF Finalapi-381321315Belum ada peringkat
- Walking AidsDokumen2 halamanWalking AidsSofia P. PanlilioBelum ada peringkat
- Map - From - SanBrunoMtnSept2014 With Devil's ArroyoDokumen1 halamanMap - From - SanBrunoMtnSept2014 With Devil's ArroyoThomas AlbinBelum ada peringkat
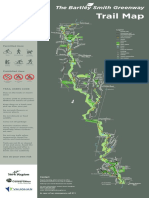
- Bartley Smith Greenway Trail MapDokumen1 halamanBartley Smith Greenway Trail MapMenandro AmbanlocBelum ada peringkat
- Forbidden Siren 2 Walk ThroughDokumen156 halamanForbidden Siren 2 Walk ThroughWahyu OetomoBelum ada peringkat
- Everyday Life in Motion. The Art of Walking in Late-Nineteenth-Century ParisDokumen25 halamanEveryday Life in Motion. The Art of Walking in Late-Nineteenth-Century ParisBudes Alexandru MihaiBelum ada peringkat
- SPEX 201 Lab 1 - Motion Analysis Techniques - STUDENT - 2023Dokumen8 halamanSPEX 201 Lab 1 - Motion Analysis Techniques - STUDENT - 2023tom mallardBelum ada peringkat
- Excel Compras y SuministrosDokumen6 halamanExcel Compras y SuministrosAlejandra CeballosBelum ada peringkat
- All Round & Beginner Climbing Shoe Comparison ChartDokumen8 halamanAll Round & Beginner Climbing Shoe Comparison ChartGonzalo Díez LazcorretaBelum ada peringkat
- Hiking and Trekking Trails in Tokyo and VicinityDokumen2 halamanHiking and Trekking Trails in Tokyo and VicinityNoemiCiullaBelum ada peringkat