Anda mungkin juga menyukai
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Attachment 3 - List of Recommended Hospital For KOICA SP Medical Check-UpDokumen36 halamanAttachment 3 - List of Recommended Hospital For KOICA SP Medical Check-UpAugustin Tadiamba PambiBelum ada peringkat
- Ntsmslka 000012Dokumen227 halamanNtsmslka 000012VinayBelum ada peringkat
- Checklist for Teaching Strategies for Learners with Special NeedsDokumen2 halamanChecklist for Teaching Strategies for Learners with Special NeedsJasmin Aldueza100% (6)
- LM340/LM78XX Series 3-Terminal Positive Regulators: General DescriptionDokumen17 halamanLM340/LM78XX Series 3-Terminal Positive Regulators: General DescriptionAlexandru Gabriel HunaBelum ada peringkat
- Angle Types Acute Right ObtuseDokumen2 halamanAngle Types Acute Right ObtuseBenjamin DennisBelum ada peringkat
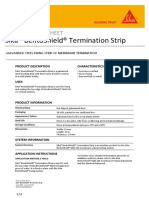
- Sika® Bentoshield® Termination Strip: Product Data SheetDokumen2 halamanSika® Bentoshield® Termination Strip: Product Data SheetKhin Sandi KoBelum ada peringkat
- Guide: Daily ReferenceDokumen8 halamanGuide: Daily ReferenceGalina TodorovaBelum ada peringkat
- Lesson 2: Problem Solving Through Flowcharts 1Dokumen14 halamanLesson 2: Problem Solving Through Flowcharts 1catherine carreonBelum ada peringkat
- Answer Sheet: Answersheet NumberDokumen1 halamanAnswer Sheet: Answersheet NumberSagar Thengil100% (1)
- The Rose Review 2009Dokumen217 halamanThe Rose Review 2009Matt Grant100% (3)
- Cast Iron Gate Valve ANSI-150 Series A1GA1-A150 - A1GA2-A150Dokumen1 halamanCast Iron Gate Valve ANSI-150 Series A1GA1-A150 - A1GA2-A150izatBelum ada peringkat
- Rl4-Ucon10 BrukermanualDokumen22 halamanRl4-Ucon10 Brukermanuallukes1582Belum ada peringkat
- EMT3-C10186 Manual (Rev. 1) W E-Stop and Throttle Pot (71610)Dokumen17 halamanEMT3-C10186 Manual (Rev. 1) W E-Stop and Throttle Pot (71610)Matias Contreras Köbrich100% (2)
- 17 Laws of TeamworkDokumen2 halaman17 Laws of TeamworkJesus Alarcon Z CantuBelum ada peringkat
- PSD1Dokumen8 halamanPSD1Naeem Ali SajadBelum ada peringkat
- Plaxis - Bearing Capacity of Strip FootingDokumen6 halamanPlaxis - Bearing Capacity of Strip FootingKasim BaručijaBelum ada peringkat
- Instruction Manual XPU-2 Option RS-232C / RS-485Dokumen12 halamanInstruction Manual XPU-2 Option RS-232C / RS-485Thái NgọcBelum ada peringkat
- (Advances in Experimental Medicine and Biology 1142) Qing Yang, Tamo Fukamizo - Targeting Chitin-Containing Organisms-Springer Singapore (2019)Dokumen293 halaman(Advances in Experimental Medicine and Biology 1142) Qing Yang, Tamo Fukamizo - Targeting Chitin-Containing Organisms-Springer Singapore (2019)La Ciencia de AlejoBelum ada peringkat
- Seleccion & Brochure Bomba Griswold BoosterDokumen19 halamanSeleccion & Brochure Bomba Griswold BoosterJonathan Mario Bolivar AldanaBelum ada peringkat
- Brinsmade, El Latifundismo Mexicano, Su Origen y Su RemedioDokumen265 halamanBrinsmade, El Latifundismo Mexicano, Su Origen y Su RemedioAnonymous iH3yyVw100% (1)
- Moon SignsDokumen2 halamanMoon SignsAdvotiya RaskolnikovaBelum ada peringkat
- Soil Investigations & Testing For The Proposed Road 1 North, Kidurong Industrial Estate (Kinda) For Bintulu Development Authority PDFDokumen8 halamanSoil Investigations & Testing For The Proposed Road 1 North, Kidurong Industrial Estate (Kinda) For Bintulu Development Authority PDFracing.phreakBelum ada peringkat
- Midlands State University Library Department Course: Information Literacy Skills (Hcs135)Dokumen7 halamanMidlands State University Library Department Course: Information Literacy Skills (Hcs135)Loveniah Yemurai MbakataBelum ada peringkat
- Waste Management Report 08 PDFDokumen7 halamanWaste Management Report 08 PDFMikeRenderBelum ada peringkat
- Affidavit of Carol Jean CoscoDokumen54 halamanAffidavit of Carol Jean CoscochchiangBelum ada peringkat
- Short Span Bridge Construction MethodDokumen41 halamanShort Span Bridge Construction Method20MK06 - PUSHPA SBelum ada peringkat
- SD ContentsDokumen18 halamanSD ContentsAnonymous gUjimJKBelum ada peringkat
- Telling Time and Telephone Communication: He O LLDokumen33 halamanTelling Time and Telephone Communication: He O LLnovaBelum ada peringkat
- CII4Q3 - Computer Vision-EAR - Week-11-Intro To Deep Learning v1.0Dokumen50 halamanCII4Q3 - Computer Vision-EAR - Week-11-Intro To Deep Learning v1.0Zee IngameBelum ada peringkat
- Answer THREE Questions.: (Part Marks)Dokumen5 halamanAnswer THREE Questions.: (Part Marks)Roy VeseyBelum ada peringkat