Anda mungkin juga menyukai
- Apert N CrouzonDokumen13 halamanApert N CrouzonfayasyabminBelum ada peringkat
- Contoh Kasus AutisDokumen3 halamanContoh Kasus AutisfayasyabminBelum ada peringkat
- Oral ScrerenDokumen9 halamanOral Screrenfayasyabmin100% (1)
- The Individually Prepared Transpalatal Arch (TPA) : Valentin Moutaftchiev, Alexander MoutaftchievDokumen4 halamanThe Individually Prepared Transpalatal Arch (TPA) : Valentin Moutaftchiev, Alexander MoutaftchievfayasyabminBelum ada peringkat
- Sag 34 1 10 0309 11 PDFDokumen8 halamanSag 34 1 10 0309 11 PDFfayasyabminBelum ada peringkat
- Sag 34 1 10 0309 11 PDFDokumen8 halamanSag 34 1 10 0309 11 PDFfayasyabminBelum ada peringkat
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5795)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Uprighting of Lower MolarsDokumen10 halamanUprighting of Lower Molarssolodont1Belum ada peringkat
- NDS Study Club Brochure v4Dokumen9 halamanNDS Study Club Brochure v4Hamed KarimiBelum ada peringkat
- Booklet - e 1 - 2013Dokumen101 halamanBooklet - e 1 - 2013Dani AedoBelum ada peringkat
- s41415 023 5624 0 LibreDokumen6 halamans41415 023 5624 0 LibreAZWATEE BINTI ABDUL AZIZBelum ada peringkat
- Coricama c17 en CatalogueDokumen232 halamanCoricama c17 en CatalogueBernythefly axcBelum ada peringkat
- Da Costa 2013, A Meta Analysis of The Most Indicated Preparation Design For Porcelain Laminate VeneersDokumen7 halamanDa Costa 2013, A Meta Analysis of The Most Indicated Preparation Design For Porcelain Laminate VeneersAaron MarroBelum ada peringkat
- A Retrospective Comparison of Two Protocols For Correction of Skeletal Class III Malocclusion in Prepubertal ChildrenDokumen11 halamanA Retrospective Comparison of Two Protocols For Correction of Skeletal Class III Malocclusion in Prepubertal ChildrenMariana SantosBelum ada peringkat
- Pitts Et Al 2019 Early Childhood Caries IAPD Bangkok Declaration. IJPDDokumen3 halamanPitts Et Al 2019 Early Childhood Caries IAPD Bangkok Declaration. IJPDThaliaBelum ada peringkat
- A Survey On Oral Health Attitude, Awareness and Behaviour of Dental StudentsDokumen5 halamanA Survey On Oral Health Attitude, Awareness and Behaviour of Dental StudentsazizahBelum ada peringkat
- The Coronally Advanced Flap in Combination With Platelet-Rich Fibrin (PRF) and Enamel Matrix Derivative in The Treatment of Gingival Recession: A Comparative StudyDokumen15 halamanThe Coronally Advanced Flap in Combination With Platelet-Rich Fibrin (PRF) and Enamel Matrix Derivative in The Treatment of Gingival Recession: A Comparative StudyAnsh Veer ChouhanBelum ada peringkat
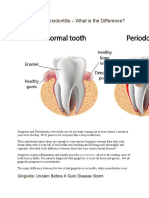
- Gingivitis Vs PeriodontitisDokumen2 halamanGingivitis Vs Periodontitisandreas kevinBelum ada peringkat
- Facebow Tech Spec Gen LRDokumen1 halamanFacebow Tech Spec Gen LRrojBelum ada peringkat
- Andrews, Will - Scientific Treatment Goals For Oral and Facial HarmonyDokumen7 halamanAndrews, Will - Scientific Treatment Goals For Oral and Facial Harmonykarol yanacBelum ada peringkat
- New Microsoft Office Word DocumentDokumen3 halamanNew Microsoft Office Word DocumentAtulsanapBelum ada peringkat
- Effect of Lip Bumpers On MandibularDokumen4 halamanEffect of Lip Bumpers On MandibularMaria SilvaBelum ada peringkat
- Upto HistoryDokumen70 halamanUpto HistoryAnil Sukumaran33% (3)
- Tsoukaki 2012Dokumen8 halamanTsoukaki 2012Marina JoelBelum ada peringkat
- Davidovitch1995 PDFDokumen6 halamanDavidovitch1995 PDFRahulLife'sBelum ada peringkat
- The Evaluation of The Nasolabial Angle in Iraqi Subject With Class I, II and III Skeletal Relationship (Comparative Study)Dokumen5 halamanThe Evaluation of The Nasolabial Angle in Iraqi Subject With Class I, II and III Skeletal Relationship (Comparative Study)Rebin AliBelum ada peringkat
- Lec 8 3rd Class PDFDokumen4 halamanLec 8 3rd Class PDFBrandon AviciiBelum ada peringkat
- RPD M C Q With AnswersDokumen23 halamanRPD M C Q With Answersيارا حسين81% (16)
- Orthodontic Treatment: Patient Information LeafletDokumen2 halamanOrthodontic Treatment: Patient Information LeafletRakan KhtoomBelum ada peringkat
- Efektivitas Pasta Gigi Herbal Dan Non-Herbal Terhadap Penurunan Plak Gigi Anak Usia 12-14 TahunDokumen7 halamanEfektivitas Pasta Gigi Herbal Dan Non-Herbal Terhadap Penurunan Plak Gigi Anak Usia 12-14 Tahunfadhilah nurBelum ada peringkat
- Dentaltrauma: Lewis C. JonesDokumen8 halamanDentaltrauma: Lewis C. JonesHusni mubarakBelum ada peringkat
- Managing Geriatric PatientsDokumen8 halamanManaging Geriatric PatientsSarah KahilBelum ada peringkat
- Surveyors &surveying Inrpd: Presented By: Annesha K. Konwar Mds Ii ND YearDokumen82 halamanSurveyors &surveying Inrpd: Presented By: Annesha K. Konwar Mds Ii ND YearArchita KureelBelum ada peringkat
- Class 7 Work Book Answers Page 16Dokumen2 halamanClass 7 Work Book Answers Page 16Gaurav SethiBelum ada peringkat
- Cavity PrepDokumen10 halamanCavity PrepShruti GolaiBelum ada peringkat
- Ferrari Et Al 2017 JDentDokumen29 halamanFerrari Et Al 2017 JDentAli Al-QaysiBelum ada peringkat
- MOH Exam Paper C PDFDokumen7 halamanMOH Exam Paper C PDFmidhun0% (1)