Anda mungkin juga menyukai
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (121)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- From Pro-Inflammatory Molecules To The Brain's Resting-State Connectivity The Future of Clinical Diagnosis of DepressionDokumen36 halamanFrom Pro-Inflammatory Molecules To The Brain's Resting-State Connectivity The Future of Clinical Diagnosis of DepressiondgavrileBelum ada peringkat
- Complications of Upper GI SDokumen30 halamanComplications of Upper GI SNavin ChandarBelum ada peringkat
- UserManual - Vitafon-2 - Edition B, IV 2015Dokumen85 halamanUserManual - Vitafon-2 - Edition B, IV 2015Tom LuxembourgeoiseBelum ada peringkat
- The BMA Family Doctor Home AdviserDokumen319 halamanThe BMA Family Doctor Home Adviservikash100% (4)
- Chloramphenicol Treatment For Acute Infective Conjunctivitis in Children in Primary Care: A Randomised Double-Blind Placebo-Controlled TrialDokumen8 halamanChloramphenicol Treatment For Acute Infective Conjunctivitis in Children in Primary Care: A Randomised Double-Blind Placebo-Controlled TrialFemi OdeBelum ada peringkat
- Systemic PathologyDokumen21 halamanSystemic PathologyAijan MurzalievaBelum ada peringkat
- Faculty of Medicine and Health Sciences Score Sheet For CASE Write-UpDokumen30 halamanFaculty of Medicine and Health Sciences Score Sheet For CASE Write-UpJared Khoo Er HauBelum ada peringkat
- Smallpox A Dead DiseaseDokumen42 halamanSmallpox A Dead DiseasefarigBelum ada peringkat
- Medicinal Flora in Holy QuranDokumen16 halamanMedicinal Flora in Holy QuranMuhammad Zakiy FadlullahBelum ada peringkat
- Pathophysiology AKI in Covid ACKD JournalDokumen30 halamanPathophysiology AKI in Covid ACKD JournalChucksters79Belum ada peringkat
- Answer Key Practice NeuroDokumen11 halamanAnswer Key Practice NeuroAnonymous iG0DCOfBelum ada peringkat
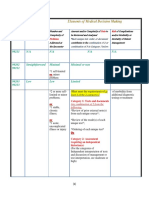
- 3-Level of MDMDokumen3 halaman3-Level of MDMmedical codingBelum ada peringkat
- #Comprehensiveclinicalcases #Surgery-Ulcer: Patient ParticularsDokumen5 halaman#Comprehensiveclinicalcases #Surgery-Ulcer: Patient ParticularsRachitha GuttaBelum ada peringkat
- Sop of Clo2Dokumen4 halamanSop of Clo2Anup RanjanBelum ada peringkat
- Clinical Neurophysiology 5Th Edition Devon I Rubin Full ChapterDokumen67 halamanClinical Neurophysiology 5Th Edition Devon I Rubin Full Chapterdoug.wiggins940100% (6)
- NURSING CARE PLAN - Liver CirrhosisDokumen2 halamanNURSING CARE PLAN - Liver Cirrhosisderic100% (27)
- Age ( 55 Years Old) - Female Sex - BMI: 28 (Overweight) - Alcohol Consumption - Uncontrolled Hypertension - High Fat DietDokumen3 halamanAge ( 55 Years Old) - Female Sex - BMI: 28 (Overweight) - Alcohol Consumption - Uncontrolled Hypertension - High Fat DietelleBelum ada peringkat
- Department of Education: Republic of The PhilippinesDokumen7 halamanDepartment of Education: Republic of The PhilippinesAngeline AtienzaBelum ada peringkat
- I Summary Family MedicineDokumen185 halamanI Summary Family MedicineModa ModyBelum ada peringkat
- Aun Herbal CatalogDokumen29 halamanAun Herbal Catalogaunherbalremedies2009Belum ada peringkat
- Neuromuscular ImagingDokumen432 halamanNeuromuscular ImagingLeticiaElizabethEchevarria100% (2)
- Assignment On Health Assessment 1Dokumen5 halamanAssignment On Health Assessment 1Sumit YadavBelum ada peringkat
- 00 TB MCQ Quiz - Eng PDFDokumen32 halaman00 TB MCQ Quiz - Eng PDFSp PpvBelum ada peringkat
- 8 - Somatic Symptoms and Dissociative DisordersDokumen32 halaman8 - Somatic Symptoms and Dissociative Disordersalaakassem424Belum ada peringkat
- Government Initiatives in Health and Nutrition: Vinod PaulDokumen29 halamanGovernment Initiatives in Health and Nutrition: Vinod PaulMani KandanBelum ada peringkat
- Concept Map Joshua ValdrizDokumen1 halamanConcept Map Joshua ValdrizJoshua ValdrizBelum ada peringkat
- Syllabus MO Dentist 020211Dokumen2 halamanSyllabus MO Dentist 020211Himanshu SainiBelum ada peringkat
- MIcrobiology Experiment 12 15Dokumen14 halamanMIcrobiology Experiment 12 15Christina SantosBelum ada peringkat
- Lecture-4 Viral GastroenteritisDokumen37 halamanLecture-4 Viral GastroenteritislolitlolatBelum ada peringkat
- Icpc PolicyDokumen45 halamanIcpc PolicyMark Emil BautistaBelum ada peringkat