Anda mungkin juga menyukai
- Bacterial Contamination.: Prepared By: Raitha R Suleiman Alexandria University 2018Dokumen13 halamanBacterial Contamination.: Prepared By: Raitha R Suleiman Alexandria University 2018Aymen OmerBelum ada peringkat
- Chronic GVHD Symptom ScaleDokumen5 halamanChronic GVHD Symptom ScaleAymen OmerBelum ada peringkat
- FigureDokumen1 halamanFigureAymen OmerBelum ada peringkat
- Estimation of Impedance Platelet Count A PDFDokumen4 halamanEstimation of Impedance Platelet Count A PDFAymen OmerBelum ada peringkat
- Normal Ranges Core HaematologyDokumen1 halamanNormal Ranges Core HaematologyAymen OmerBelum ada peringkat
- A GVHDDokumen40 halamanA GVHDAymen Omer100% (1)
- Haploidentical Stem Cell Transplant: Zeina Al-Mansour, MDDokumen22 halamanHaploidentical Stem Cell Transplant: Zeina Al-Mansour, MDAymen OmerBelum ada peringkat
- Varient CML BCR-ABL PositiveDokumen11 halamanVarient CML BCR-ABL PositiveAymen OmerBelum ada peringkat
- Seek Crit Care 26 Sample NewDokumen6 halamanSeek Crit Care 26 Sample NewAymen OmerBelum ada peringkat
- Cardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingDokumen46 halamanCardio Vascular Assessment: Manali H Solanki F.Y.M.Sc - Nursing J G College of NursingmeghanaBelum ada peringkat
- Transplantation &: Tissue RejectionDokumen15 halamanTransplantation &: Tissue RejectionAymen OmerBelum ada peringkat
- Diagnosis and Management of Polycythaemia VeraDokumen16 halamanDiagnosis and Management of Polycythaemia VeraAymen OmerBelum ada peringkat
- Hepatitsppt 151223190415Dokumen26 halamanHepatitsppt 151223190415Aymen OmerBelum ada peringkat
- Testicular Feminization Syndrome TFM: Ruslan Bayramov .MD Medical Genetics Department Erciyes UniversityDokumen25 halamanTesticular Feminization Syndrome TFM: Ruslan Bayramov .MD Medical Genetics Department Erciyes UniversityAymen OmerBelum ada peringkat
- Hypercalcaemia and Hypercalciuria: JamieDokumen11 halamanHypercalcaemia and Hypercalciuria: JamieAymen OmerBelum ada peringkat
- Hepatitis C Virus: Section: 3Dokumen43 halamanHepatitis C Virus: Section: 3Aymen OmerBelum ada peringkat
- A Guideline For The Diagnosis and Management of Polycythaemia VeraDokumen23 halamanA Guideline For The Diagnosis and Management of Polycythaemia VeraAymen OmerBelum ada peringkat
- Aml 1Dokumen2 halamanAml 1Aymen OmerBelum ada peringkat
- Biochemistrypresentation Copy 150905173417 Lva1 App6892Dokumen20 halamanBiochemistrypresentation Copy 150905173417 Lva1 App6892Dawlat SalamaBelum ada peringkat
- 9123633Dokumen99 halaman9123633Aymen OmerBelum ada peringkat
- Hepatorenal SyndromeDokumen4 halamanHepatorenal SyndromeAymen OmerBelum ada peringkat
- Basic Epidemiologic and Biostatistical Terminology ForDokumen15 halamanBasic Epidemiologic and Biostatistical Terminology ForAymen OmerBelum ada peringkat
- Some Biochem MnemonicsDokumen8 halamanSome Biochem MnemonicsMikey PalominoBelum ada peringkat
- Surviving 4th Year MedicineDokumen64 halamanSurviving 4th Year MedicineAymen OmerBelum ada peringkat
- Guidelines For The Use of Fresh-Frozen Plasma, Cryoprecipitate & CryosupernantDokumen18 halamanGuidelines For The Use of Fresh-Frozen Plasma, Cryoprecipitate & CryosupernantAymen OmerBelum ada peringkat
- Extrinsic PathwayDokumen1 halamanExtrinsic PathwayAymen OmerBelum ada peringkat
- Study of The Pattern of Chest Diseases Including Tuberculosis in Qena Chest HospitalDokumen10 halamanStudy of The Pattern of Chest Diseases Including Tuberculosis in Qena Chest HospitalAymen OmerBelum ada peringkat
- 4-27 8am Halder - Cutaneous Manif. of Diseases2Dokumen12 halaman4-27 8am Halder - Cutaneous Manif. of Diseases2Aymen OmerBelum ada peringkat
- Structure of The Protocol 2Dokumen10 halamanStructure of The Protocol 2Aymen OmerBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5782)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- ANRAP Announcement PDFDokumen1 halamanANRAP Announcement PDFBuddhi Bal ChidiBelum ada peringkat
- Dosages and Flow Rates and Pediatric Drug Administration AssignmentDokumen6 halamanDosages and Flow Rates and Pediatric Drug Administration AssignmentNavin Barnwal0% (1)
- Module 1 PHPDokumen4 halamanModule 1 PHPGE SalenBelum ada peringkat
- Cognitive Behavioral Therapy For Managing PainDokumen3 halamanCognitive Behavioral Therapy For Managing PainJustus K GatheruBelum ada peringkat
- Chapter Quiz for Antimicrobial AgentsDokumen1 halamanChapter Quiz for Antimicrobial AgentsIrwan M. IskoberBelum ada peringkat
- Tratamiento para UPP en FisioterapiaDokumen44 halamanTratamiento para UPP en FisioterapiaKimberly GomezBelum ada peringkat
- Strategies For Dengue Control ProgramDokumen22 halamanStrategies For Dengue Control ProgramNaseem QaziBelum ada peringkat
- Ling Zhi Stimulates Lymphocyte Proliferation and Modulates Con A Induced ResponseDokumen60 halamanLing Zhi Stimulates Lymphocyte Proliferation and Modulates Con A Induced Responseravee_23Belum ada peringkat
- Comminuted Patella FracturesDokumen8 halamanComminuted Patella FracturesKirana lupitaBelum ada peringkat
- Partograph in LaborDokumen3 halamanPartograph in Laborboks9s.9escaladaBelum ada peringkat
- Multiple Choice Questions For DR DoobayDokumen10 halamanMultiple Choice Questions For DR DoobaynathanielBelum ada peringkat
- Shock HypovolemicDokumen19 halamanShock HypovolemicChance Jackson100% (1)
- A Case Study On Tamaka Swasa W. S. R To Bronchial Asthma AyurvedaDokumen2 halamanA Case Study On Tamaka Swasa W. S. R To Bronchial Asthma AyurvedaInternational Journal of Innovative Science and Research TechnologyBelum ada peringkat
- Clinical Exam of The Psychiatric PX HX MSE Signs Symptoms Modified For Senior Clerks 2021Dokumen139 halamanClinical Exam of The Psychiatric PX HX MSE Signs Symptoms Modified For Senior Clerks 2021Rakesh KumarBelum ada peringkat
- StarHealthAssureInsurancePolicy BrochureDokumen13 halamanStarHealthAssureInsurancePolicy Brochurepradosh002Belum ada peringkat
- Ovarian CancerDokumen34 halamanOvarian CancerHealth Education Library for People100% (4)
- Biliary Enteric BypassDokumen25 halamanBiliary Enteric BypassAlexandru Ferdohleb100% (1)
- Battlefield Acupuncture: Rapid Pain Relief Using Semi Permanent Auricular (Ear) NeedlesDokumen4 halamanBattlefield Acupuncture: Rapid Pain Relief Using Semi Permanent Auricular (Ear) NeedlesBranko SavicBelum ada peringkat
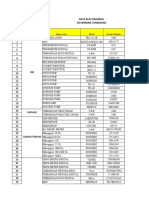
- Data Alat Kalibrasi Rs TNGDokumen10 halamanData Alat Kalibrasi Rs TNGHelena LowaBelum ada peringkat
- NURS 2003H Nursing Therapeutics & Disease ConditionsDokumen7 halamanNURS 2003H Nursing Therapeutics & Disease Conditionsgreat146Belum ada peringkat
- Reservoir Bag Physics J PhilipDokumen44 halamanReservoir Bag Physics J PhilipJashim JumliBelum ada peringkat
- Scrotal Swelling Causes and TreatmentsDokumen63 halamanScrotal Swelling Causes and TreatmentsTommysBelum ada peringkat
- Ad-Din Medical College Hospital: List of DoctorsDokumen5 halamanAd-Din Medical College Hospital: List of DoctorsKulfi BarfiBelum ada peringkat
- 0007BDokumen12 halaman0007BnacerBelum ada peringkat
- Abbott 26090 CAG Brochure r2 ZincDokumen24 halamanAbbott 26090 CAG Brochure r2 ZinctheresmariajBelum ada peringkat
- Become A VeterinarianDokumen6 halamanBecome A VeterinarianImran KhanBelum ada peringkat
- OMSC First Aid & Water Safety Activities DocumentDokumen4 halamanOMSC First Aid & Water Safety Activities DocumentPablito GuacheBelum ada peringkat
- Deep Brain Stimulation For Treatment-Resistant Depression - Efficacy, Safety and Mechanisms of ActionDokumen14 halamanDeep Brain Stimulation For Treatment-Resistant Depression - Efficacy, Safety and Mechanisms of ActionDiego SantanaBelum ada peringkat
- Essentials of Oral MedicineDokumen389 halamanEssentials of Oral MedicineKishendran R GanandranBelum ada peringkat
- Laser Retinopexy PDFDokumen4 halamanLaser Retinopexy PDFveerroxxBelum ada peringkat