Anda mungkin juga menyukai
- Medication Fact Book for Psychiatric Practice, Fifth EditionDari EverandMedication Fact Book for Psychiatric Practice, Fifth EditionBelum ada peringkat
- The Maudsley Prescribing Guidelines in PsychiatryDari EverandThe Maudsley Prescribing Guidelines in PsychiatryPenilaian: 5 dari 5 bintang5/5 (1)
- Psychotherapeutic Drugs: Pam Pam LamDokumen7 halamanPsychotherapeutic Drugs: Pam Pam Lamchubbygunny_29776413Belum ada peringkat
- Psychotropic Medication ReviewDokumen7 halamanPsychotropic Medication ReviewAakash Shah100% (1)
- Anti Depressants FinalDokumen61 halamanAnti Depressants FinalAuthor Nauman Shad100% (1)
- Psycho PharmaDokumen8 halamanPsycho PharmaMark JosephBelum ada peringkat
- Psychiatry Pharmacology J. Psychiatry' AntidepressantsDokumen9 halamanPsychiatry Pharmacology J. Psychiatry' AntidepressantssumithjalyBelum ada peringkat
- Shortened REM Latency and Increased REM: Previous AttemptDokumen19 halamanShortened REM Latency and Increased REM: Previous AttemptActeen MyoseenBelum ada peringkat
- Antidepressants and AntipsychoticsDokumen8 halamanAntidepressants and AntipsychoticsWillBelum ada peringkat
- Drug List Psych Optho NeuroDokumen22 halamanDrug List Psych Optho NeuroAshley BarrileBelum ada peringkat
- Generics Antidepressants Comparison Chart PDFDokumen2 halamanGenerics Antidepressants Comparison Chart PDFYazirBelum ada peringkat
- Psychiatric Study GuideDokumen18 halamanPsychiatric Study Guiderebeccacampbell100% (1)
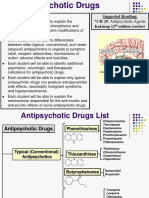
- AntipsychoticsDokumen10 halamanAntipsychoticswawing16Belum ada peringkat
- Medication Conversion ChartDokumen2 halamanMedication Conversion ChartIlinca mirnoviciBelum ada peringkat
- Geriatric Giants - DR SeymourDokumen108 halamanGeriatric Giants - DR SeymourSharon Mallia100% (1)
- Provisional: Borderline Personality Disorder Differential DXDokumen6 halamanProvisional: Borderline Personality Disorder Differential DXhernandez2812Belum ada peringkat
- Handbook of Psychiatric DrugsDokumen68 halamanHandbook of Psychiatric Drugsbson100% (13)
- Table 1: Substrates of Cytochrome P450 (CYP) EnzymesDokumen6 halamanTable 1: Substrates of Cytochrome P450 (CYP) EnzymesNurul Kamilah SadliBelum ada peringkat
- Neurotransmitter Pathway in PsychiatryDokumen22 halamanNeurotransmitter Pathway in PsychiatryameerBelum ada peringkat
- Mental Disorders Due To A General Medical ConditionDokumen145 halamanMental Disorders Due To A General Medical ConditionKaye NepomucenoBelum ada peringkat
- Antidepressant DrugsDokumen21 halamanAntidepressant DrugsKashis SharmaBelum ada peringkat
- Review of Antipsychotic DrugsDokumen15 halamanReview of Antipsychotic DrugsTuanthonBoonlue100% (1)
- Clozapine Prescriber GuideDokumen17 halamanClozapine Prescriber GuideNicolás Ariel LescanoBelum ada peringkat
- Treatment Modalities For Mood DisordersDokumen55 halamanTreatment Modalities For Mood DisordersGlory MimiBelum ada peringkat
- Handy Summary Chart Comparing The Main Medications For DepressionDokumen2 halamanHandy Summary Chart Comparing The Main Medications For Depressionrowanpurdy100% (4)
- (OS 213) LEC 03 Drugs Acting On The Respiratory System (1) - 1Dokumen16 halaman(OS 213) LEC 03 Drugs Acting On The Respiratory System (1) - 1Yavuz DanisBelum ada peringkat
- Antidepressant Side Effects 2006Dokumen9 halamanAntidepressant Side Effects 2006Renny AnggrainiBelum ada peringkat
- Overview of Psychotropic DrugsDokumen7 halamanOverview of Psychotropic Drugsnad101Belum ada peringkat
- Treatment-Resistant Obsessive-Compulsive Disorder (OCD) - Current UnderstandingDokumen21 halamanTreatment-Resistant Obsessive-Compulsive Disorder (OCD) - Current UnderstandingRapapportBelum ada peringkat
- Medical Student Psychopharmacology - PPTX 2015-16 John WDokumen99 halamanMedical Student Psychopharmacology - PPTX 2015-16 John WMrLarry DolorBelum ada peringkat
- Antidepressant Use in Adults With Chronic Kidney DiseaseDokumen1 halamanAntidepressant Use in Adults With Chronic Kidney DiseaseAzhar Ali100% (1)
- List of Books: S.N Author Title Publication ISBN QTY RemarkDokumen2 halamanList of Books: S.N Author Title Publication ISBN QTY RemarkTemesgen EndalewBelum ada peringkat
- Neuroleptics & AnxiolyticsDokumen65 halamanNeuroleptics & AnxiolyticsAntonPurpurovBelum ada peringkat
- StahleDokumen12 halamanStahlekhaledazima0% (2)
- High Yield Psychiatry: Shelf Exam Review Emma Holliday RamahiDokumen43 halamanHigh Yield Psychiatry: Shelf Exam Review Emma Holliday Ramahigreg100% (1)
- Handy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Dokumen3 halamanHandy Hints When Prescribing Antidepressants: Selective Serotonin Reuptake Inhibitors (Ssris)Mariya ZhekovaBelum ada peringkat
- Psych DrugsDokumen3 halamanPsych DrugsSwarna BanikBelum ada peringkat
- Antidepressant Therapy Algorithm PDFDokumen12 halamanAntidepressant Therapy Algorithm PDFiwul kiwul KriwulBelum ada peringkat
- Antipsychotic DrugsDokumen47 halamanAntipsychotic DrugsIkram UddinBelum ada peringkat
- CEP BPSD Discussion Guide ENG RFCG Updated2019 PDFDokumen8 halamanCEP BPSD Discussion Guide ENG RFCG Updated2019 PDFM.DalaniBelum ada peringkat
- AntipsychoticsDokumen4 halamanAntipsychoticsRana MuhammadBelum ada peringkat
- Pharmacology (Psychosis and Mania)Dokumen53 halamanPharmacology (Psychosis and Mania)lavanyakakarlaBelum ada peringkat
- Pharmacotherapy in PschiatryDokumen8 halamanPharmacotherapy in PschiatryygfhdgBelum ada peringkat
- DR - Usama.mahmoud Psychiatry - Notes MSDokumen64 halamanDR - Usama.mahmoud Psychiatry - Notes MSMariam A. KarimBelum ada peringkat
- Psychopharma 1Dokumen7 halamanPsychopharma 1Mitchee Zialcita100% (1)
- Antidepressant Medication ChartDokumen2 halamanAntidepressant Medication Chartbabaran2Belum ada peringkat
- PA 644 - M2 LecturesDokumen412 halamanPA 644 - M2 LectureskatBelum ada peringkat
- Antipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationDokumen6 halamanAntipsychotic Medication: Generic Name Trade Name Indications Contraindications Drug Interaction Side Effects Nursing ImplicationJaylord VerazonBelum ada peringkat
- Sudden Onset (Within 2 Weeks) of at Least One of TheDokumen2 halamanSudden Onset (Within 2 Weeks) of at Least One of TheNeicole BandalaBelum ada peringkat
- PsychopharmacologyDokumen64 halamanPsychopharmacologyGaurav Tandon100% (2)
- Benzodiazepine Comparison Chart - Commonly Available Sedative Hypnotic Anti Anxiety (Anxiolytic) Anti Epileptic MedicationsDokumen2 halamanBenzodiazepine Comparison Chart - Commonly Available Sedative Hypnotic Anti Anxiety (Anxiolytic) Anti Epileptic MedicationsChristopher Chrysostom100% (3)
- Antipsychotics: Corina Freitas MS, MD, MBA, DABFMDokumen48 halamanAntipsychotics: Corina Freitas MS, MD, MBA, DABFMCorina FreitasBelum ada peringkat
- Bipolar DisorderDokumen1 halamanBipolar DisorderNur BalqisBelum ada peringkat
- 4.2 Psychotropic Drugs Used in PsychiatryDokumen32 halaman4.2 Psychotropic Drugs Used in PsychiatryAmar Nur Arif ZazuliBelum ada peringkat
- AntipsychoticsDokumen29 halamanAntipsychoticsTyler Lawrence Coye100% (5)
- Handy Summary Chart Comparing The Main Medications For PsychosisDokumen3 halamanHandy Summary Chart Comparing The Main Medications For Psychosisrowanpurdy100% (2)
- Exam 1 2Dokumen18 halamanExam 1 2api-444187370Belum ada peringkat
- Emergency Psychiatry Other Than Suicide: Dr. Pooja Singh, MD Assistant ProfessorDokumen45 halamanEmergency Psychiatry Other Than Suicide: Dr. Pooja Singh, MD Assistant Professorpooja singhBelum ada peringkat
- Malingering in Psychiatric DisordersDokumen4 halamanMalingering in Psychiatric DisordersStuti JoshiBelum ada peringkat
- 5 Minute Guide Electricity StorageDokumen17 halaman5 Minute Guide Electricity StorageCarlos HolguinBelum ada peringkat
- Structure of Atoms-11th Cbse Text AnswersDokumen33 halamanStructure of Atoms-11th Cbse Text AnswersKalai VananBelum ada peringkat
- Pharmacognostical and Preliminary Phytochemical Screening On Leaves of Trianthema Decandra Linn.Dokumen3 halamanPharmacognostical and Preliminary Phytochemical Screening On Leaves of Trianthema Decandra Linn.anto_pharma7784Belum ada peringkat
- Cbse Class 10 Science SyllabusDokumen2 halamanCbse Class 10 Science Syllabusराहुल रविराजBelum ada peringkat
- ETT Seminar - Isotopes in MedicineDokumen71 halamanETT Seminar - Isotopes in MedicineisocenterBelum ada peringkat
- Bioconversion of Fish Waste Into A Liquid Fertilizer and Its Impact On Semi - Arid Tropical Crops. 2020Dokumen10 halamanBioconversion of Fish Waste Into A Liquid Fertilizer and Its Impact On Semi - Arid Tropical Crops. 2020José Antonio MaquénBelum ada peringkat
- Carbon Dioxide Capture by Amines Increasing The Efficiency by Amine Structure Modification PDFDokumen2 halamanCarbon Dioxide Capture by Amines Increasing The Efficiency by Amine Structure Modification PDFJorgeSantosAquinoBelum ada peringkat
- EagleBurgmann MG1 enDokumen4 halamanEagleBurgmann MG1 ensanjeevvangeBelum ada peringkat
- Who We Are: Case Study-Mahindra ChlorisDokumen25 halamanWho We Are: Case Study-Mahindra ChlorisSUNIDHI VERMABelum ada peringkat
- Assignment 07 ADokumen3 halamanAssignment 07 AsundusBelum ada peringkat
- J.ultsonch.2014.08.022 InglesDokumen48 halamanJ.ultsonch.2014.08.022 InglesBrayan LuisBelum ada peringkat
- Gravimetric Analysis Laboratory ReportDokumen9 halamanGravimetric Analysis Laboratory ReportShawn RizalBelum ada peringkat
- Chemical Compositions of Banana Peels (Musa Sapientum) Fruits Cultivated in Malaysia Using Proximate AnalysisDokumen6 halamanChemical Compositions of Banana Peels (Musa Sapientum) Fruits Cultivated in Malaysia Using Proximate AnalysiszawBelum ada peringkat
- UO-II Chapter 4 (Adsorption)Dokumen27 halamanUO-II Chapter 4 (Adsorption)Ghaydah Hamed Rashid Al-AbriBelum ada peringkat
- InternshipDokumen16 halamanInternshipSarthak SinghBelum ada peringkat
- 3.AcidBases FinalDokumen35 halaman3.AcidBases FinalSoham RaneBelum ada peringkat
- Type of Chemical ReactionsDokumen13 halamanType of Chemical ReactionsSAHARAN ANANDBelum ada peringkat
- Regents Homeostasis and EnzymesDokumen5 halamanRegents Homeostasis and Enzymesapi-3031203990% (1)
- Whitmore Decathlon Gold Open Gear LubricantDokumen1 halamanWhitmore Decathlon Gold Open Gear LubricantDon HowardBelum ada peringkat
- Four Factors Affecting The Rate of Chemical ReactionDokumen5 halamanFour Factors Affecting The Rate of Chemical ReactionFeliciano Tristan E.Belum ada peringkat
- Artificial Blood: Dr. Pragasam Viswanathan, Professor, SBSTDokumen21 halamanArtificial Blood: Dr. Pragasam Viswanathan, Professor, SBSTMaru Mengesha Worku 18BBT0285Belum ada peringkat
- Auditor or ManagerDokumen7 halamanAuditor or Managerapi-79118648Belum ada peringkat
- Experiment A Test For Lipid Result: Result When Added To WaterDokumen5 halamanExperiment A Test For Lipid Result: Result When Added To WaterSuu Wan0% (2)
- IGNTU Econtent 674613883400 B.SC EnvironmentalSciences 2 PallaviDas EnvironmentalPollutionandHumanHealth 2Dokumen136 halamanIGNTU Econtent 674613883400 B.SC EnvironmentalSciences 2 PallaviDas EnvironmentalPollutionandHumanHealth 2Neeraj Raushan KanthBelum ada peringkat
- 444 Data SheetDokumen2 halaman444 Data SheetSabareesh MylsamyBelum ada peringkat
- Cell Wall: Presented by M. Vijaya LakshmiDokumen9 halamanCell Wall: Presented by M. Vijaya LakshmiATCHUNALA SAIBelum ada peringkat
- Bet MethodDokumen16 halamanBet MethodG Nivetha100% (1)
- Hydro Silk Fluid Englisch 06 2020Dokumen1 halamanHydro Silk Fluid Englisch 06 2020Saman KhalidBelum ada peringkat
- Microscope: Trace Evidence PowerpointDokumen17 halamanMicroscope: Trace Evidence PowerpointCarlos A. Aponte OteroBelum ada peringkat
- Aladin 2017Dokumen6 halamanAladin 2017Dwi ermawatiBelum ada peringkat