Anda mungkin juga menyukai
- Alcohol Withdrawal Care PlanDokumen1 halamanAlcohol Withdrawal Care PlanVanessaMUellerBelum ada peringkat
- Physical Assessment ChartDokumen1 halamanPhysical Assessment ChartVanessaMUellerBelum ada peringkat
- Lab Values Chart GuideDokumen5 halamanLab Values Chart GuideVanessaMUeller100% (3)
- Admission Database PDFDokumen6 halamanAdmission Database PDFVanessaMUellerBelum ada peringkat
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDokumen1 halamanFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerBelum ada peringkat
- Updated Clinical SheetDokumen1 halamanUpdated Clinical SheetVanessaMUellerBelum ada peringkat
- Name Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXDokumen1 halamanName Age Room Code Dr. Isolation Activity Diet Allergy: DX: HXVanessaMUellerBelum ada peringkat
- Nurse Brain Sheet Half SizeDokumen1 halamanNurse Brain Sheet Half Sizevsosa624Belum ada peringkat
- Penuemonia Care PalnDokumen2 halamanPenuemonia Care PalnVanessaMUellerBelum ada peringkat
- Fluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitDokumen1 halamanFluid/Electrolyte Imbalance S/S Nursing Care Fluid DeficitVanessaMUellerBelum ada peringkat
- Example 1 - Focus: Nausea Related To AnestheticDokumen1 halamanExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerBelum ada peringkat
- ManagmentDokumen1 halamanManagmentVanessaMUellerBelum ada peringkat
- IV PushDokumen3 halamanIV PushVanessaMUeller100% (1)
- AssessingWounds ProcedureDokumen3 halamanAssessingWounds ProcedureVanessaMUellerBelum ada peringkat
- Newborn Assessment NORMALDokumen2 halamanNewborn Assessment NORMALVanessaMUellerBelum ada peringkat
- Nurse Brain Sheet Half SizeDokumen1 halamanNurse Brain Sheet Half SizeRobyn GrogitskyBelum ada peringkat
- Diseases With Dermatologic ManifestationsDokumen1 halamanDiseases With Dermatologic ManifestationsVanessaMUellerBelum ada peringkat
- Alcohol Withdrawal Care PlanDokumen1 halamanAlcohol Withdrawal Care PlanVanessaMUeller100% (1)
- Wound Care PDFDokumen100 halamanWound Care PDFVanessaMUellerBelum ada peringkat
- COPD Care PLAN PDFDokumen2 halamanCOPD Care PLAN PDFVanessaMUeller100% (1)
- Clinical AssessementDokumen2 halamanClinical AssessementVanessaMUellerBelum ada peringkat
- AdmimDokumen2 halamanAdmimVanessaMUellerBelum ada peringkat
- Example 1 - Focus: Nausea Related To AnestheticDokumen1 halamanExample 1 - Focus: Nausea Related To AnestheticVanessaMUellerBelum ada peringkat
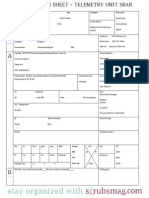
- Nurse Brain Sheet Telemetry Unit SBARDokumen1 halamanNurse Brain Sheet Telemetry Unit SBARvsosa624Belum ada peringkat
- (Chapter 3) : Cell BiologyDokumen80 halaman(Chapter 3) : Cell BiologyVanessaMUellerBelum ada peringkat
- HR Ocampo Danilo s2 E10 PDFDokumen4 halamanHR Ocampo Danilo s2 E10 PDFVanessaMUellerBelum ada peringkat
- Medication Guide with Side Effects and UsesDokumen10 halamanMedication Guide with Side Effects and UsesVanessaMUellerBelum ada peringkat
- Wound Care PDFDokumen100 halamanWound Care PDFVanessaMUeller100% (2)
- Nurse Brain Sheet With Shift HoursDokumen2 halamanNurse Brain Sheet With Shift HoursLauren Cournoyer Foreman100% (4)
- Comprehensive Head To Toe Assessment PDFDokumen22 halamanComprehensive Head To Toe Assessment PDFVanessaMUellerBelum ada peringkat
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeDari EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifePenilaian: 4 dari 5 bintang4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)Dari EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Penilaian: 4 dari 5 bintang4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItDari EverandNever Split the Difference: Negotiating As If Your Life Depended On ItPenilaian: 4.5 dari 5 bintang4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeDari EverandShoe Dog: A Memoir by the Creator of NikePenilaian: 4.5 dari 5 bintang4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerDari EverandThe Emperor of All Maladies: A Biography of CancerPenilaian: 4.5 dari 5 bintang4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceDari EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RacePenilaian: 4 dari 5 bintang4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingDari EverandThe Little Book of Hygge: Danish Secrets to Happy LivingPenilaian: 3.5 dari 5 bintang3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnDari EverandTeam of Rivals: The Political Genius of Abraham LincolnPenilaian: 4.5 dari 5 bintang4.5/5 (234)
- Grit: The Power of Passion and PerseveranceDari EverandGrit: The Power of Passion and PerseverancePenilaian: 4 dari 5 bintang4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaDari EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaPenilaian: 4.5 dari 5 bintang4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryDari EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryPenilaian: 3.5 dari 5 bintang3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealDari EverandOn Fire: The (Burning) Case for a Green New DealPenilaian: 4 dari 5 bintang4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureDari EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FuturePenilaian: 4.5 dari 5 bintang4.5/5 (474)
- Rise of ISIS: A Threat We Can't IgnoreDari EverandRise of ISIS: A Threat We Can't IgnorePenilaian: 3.5 dari 5 bintang3.5/5 (137)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersDari EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersPenilaian: 4.5 dari 5 bintang4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaDari EverandThe Unwinding: An Inner History of the New AmericaPenilaian: 4 dari 5 bintang4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyDari EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyPenilaian: 3.5 dari 5 bintang3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreDari EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You ArePenilaian: 4 dari 5 bintang4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)Dari EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Penilaian: 4.5 dari 5 bintang4.5/5 (119)
- Her Body and Other Parties: StoriesDari EverandHer Body and Other Parties: StoriesPenilaian: 4 dari 5 bintang4/5 (821)
- Clinical behavior analysis and RFT: Conceptualizing psychopathology and its treatmentDokumen28 halamanClinical behavior analysis and RFT: Conceptualizing psychopathology and its treatmentAnne de AndradeBelum ada peringkat
- Technical Bro A4 UK LR NEW v2Dokumen45 halamanTechnical Bro A4 UK LR NEW v2Roxana NegoitaBelum ada peringkat
- MAN 2 Model Medan Introduction to School Environment ReportDokumen45 halamanMAN 2 Model Medan Introduction to School Environment ReportdindaBelum ada peringkat
- EVS XT2+ Tech Ref Software Manual v10.03 PDFDokumen80 halamanEVS XT2+ Tech Ref Software Manual v10.03 PDFgibonulBelum ada peringkat
- Padmavati Gora BadalDokumen63 halamanPadmavati Gora BadalLalit MishraBelum ada peringkat
- As 2710-1984 Screw Gauges - VerificationDokumen7 halamanAs 2710-1984 Screw Gauges - VerificationSAI Global - APACBelum ada peringkat
- JKR Specs L-S1 Addendum No 1 LED Luminaires - May 2011Dokumen3 halamanJKR Specs L-S1 Addendum No 1 LED Luminaires - May 2011Leong KmBelum ada peringkat
- Math 2 Unit 9 - Probability: Lesson 1: "Sample Spaces, Subsets, and Basic Probability"Dokumen87 halamanMath 2 Unit 9 - Probability: Lesson 1: "Sample Spaces, Subsets, and Basic Probability"Anonymous BUG9KZ3100% (1)
- Osprey, Men-At-Arms #008 The Black Watch (1971) (-) OCR 8.12Dokumen48 halamanOsprey, Men-At-Arms #008 The Black Watch (1971) (-) OCR 8.12mancini100% (4)
- Adjutant-Introuvable BASIC VERSIONDokumen7 halamanAdjutant-Introuvable BASIC VERSIONfurrypdfBelum ada peringkat
- Event ReportDokumen2 halamanEvent Reportakshitdaharwal997Belum ada peringkat
- Karate Writing AssessmentDokumen2 halamanKarate Writing AssessmentLeeann RandallBelum ada peringkat
- Double Burden of Malnutrition 2017Dokumen31 halamanDouble Burden of Malnutrition 2017Gîrneţ AlinaBelum ada peringkat
- Types of Ego?Dokumen2 halamanTypes of Ego?S.UdhayakumarBelum ada peringkat
- TiONA 592 PDS - ENDokumen1 halamanTiONA 592 PDS - ENQuang VABelum ada peringkat
- Valentine Gifting - Accessories EditionDokumen25 halamanValentine Gifting - Accessories EditionPriyanath PaulBelum ada peringkat
- Auerbach Slideshow How To Write A ParagraphDokumen22 halamanAuerbach Slideshow How To Write A ParagraphFreakmaggotBelum ada peringkat
- Readme cljM880fw 2305076 518488 PDFDokumen37 halamanReadme cljM880fw 2305076 518488 PDFjuan carlos MalagonBelum ada peringkat
- SFA160Dokumen5 halamanSFA160scamalBelum ada peringkat
- Joy Difuntorum-Ramirez CVDokumen2 halamanJoy Difuntorum-Ramirez CVJojoi N JecahBelum ada peringkat
- Cls A310 Operations ManualDokumen23 halamanCls A310 Operations ManualAntonio Ahijado Mendieta100% (2)
- ECE 4400 Performance Analysis Local Computer Networks HomeworkDokumen2 halamanECE 4400 Performance Analysis Local Computer Networks HomeworkNguyen Phi HungBelum ada peringkat
- ENVPEP1412003Dokumen5 halamanENVPEP1412003south adventureBelum ada peringkat
- Chick Lit: It's not a Gum, it's a Literary TrendDokumen2 halamanChick Lit: It's not a Gum, it's a Literary TrendspringzmeBelum ada peringkat
- All Types of Switch CommandsDokumen11 halamanAll Types of Switch CommandsKunal SahooBelum ada peringkat
- Product Differentiation and Market Segmentation As Alternative Marketing StrategiesDokumen7 halamanProduct Differentiation and Market Segmentation As Alternative Marketing StrategiesCaertiMBelum ada peringkat
- Prperman 2016 14 3 (Spec. 14Dokumen8 halamanPrperman 2016 14 3 (Spec. 14celia rifaBelum ada peringkat
- Calibration GuideDokumen8 halamanCalibration Guideallwin.c4512iBelum ada peringkat
- Gabriel Nobre de Souza - Groningen Mini-MetropolisDokumen9 halamanGabriel Nobre de Souza - Groningen Mini-MetropolisGabrielNobredeSouzaBelum ada peringkat
- Kashmira Karim Charaniya's ResumeDokumen3 halamanKashmira Karim Charaniya's ResumeMegha JainBelum ada peringkat